
Gaussian, Hermite-Gaussian, and Laguerre-Gaussian beams - hermite gaussian modes
In the consultation, we will find that the corneal spherical aberration varies greatly among individuals, especially in the presence of pathological corneas or modified ones by post-refractive surgery. In a myopic treatment with excimer laser, a central flattening of the cornea is induced, generating an oblate cornea, more flat in the center than in the periphery, inducing a positive spherical aberration. In contrast, a hypermetropic correction increases the central curvature of the anterior surface of the cornea, generating a hyperprolate cornea, inducing greater negative spherical aberration that may contraindicate the use of an aspheric intraocular lens, which instead of correcting would worsen the existing spherical negative aberration, deteriorating the quality of vision.
The word “aspheric” is used to describe a surface or in this case a lens that does not have a spherical shape. In an aspherical lens, the rays of light passing through the center do not focus at the same point as the rays passing through the periphery of the lens.
by I Cordero · 2010 · Cited by 6 — Steps · Always remove dust first! · To remove stains, use a lint-free cotton swab or a lens-cleaning tissue dipped in the optical cleaning solution. · To remove ...
Spherical aberrationin a lens
If you're someone who spends a lot of time in front of screens, or works in bright environments, you might want to consider investing in some anti-glare glasses. These glasses are perfect for computer users, gamers, office workers, and even drivers who frequently encounter bright light conditions.
Today the goal of cataract surgery is to provide patients with the best possible quality of vision. While it is common to see patients post-cataract surgery with a visual acuity (VA) of 20/20, many patients remain dissatisfied with their quality of vision. This is due to several factors, including problems with the ocular surface, pseudophakic dysphotopsia, and optical aberrations in general.
1. Oshika T, et al. Influence of pupil diameter on the relation between ocular higher-order aberration and contrast sensitivity after laser in situ keratomileusis. Invest Ophthalmol Vis Sci. 2006;47:1334–8.2. Guirao A. Optical aberrations of the human cornea as a function of age. J Opt Soc Am A Opt Image Sci Vis. 2000;17:1697–702.3. Grimson JM, et al. Contrast sensitivity: establishing normative data for use in screening prospective naval pilots. Aviat Space Environ Med. 2002;73:28–35.4. Portney V. New bi-sign aspheric IOL and its application. Optom Vis Sci. 2012;89:80–9.5. Piracha AR. Using angle alpha in premium IOL screening. Cataract & Refractive Surgery Today. 2016;(3):24–25.
Spherical aberrationcause
For other uses, see Contrast. Contrast is the difference in luminance or color that makes an object (or its representation in an image or display) visible ...
It is important to note that wearing anti-glare glasses does not guarantee perfect vision. These glasses will help reduce the amount of glare, but they cannot correct any existing vision problems.
Anti-glare glasses can certainly help improve visibility while driving at night by reducing the amount of glare from headlights and streetlights. However, it's important to keep in mind that they aren't specifically designed for night driving. Other factors such as the colour and brightness of the lenses, the shape of the lenses, and the lighting conditions can also play a role in visibility and safety while on the road.
Naturally, the human cornea is aspheric, usually a bit more curved in the center and flattened toward the periphery; we call this form “prolate.” In a prolated cornea, the rays of light that cross the center of the cornea tend to converge or focus on a point anterior to the peripheral rays, and this aberration is called “negative spherical aberration.” In an oblate cornea, the central light rays are focused behind the peripheral rays, and this aberration is called “positive spherical aberration” (Figure 1).
Spherical aberrationand chromaticaberration
How do they work you might ask? Well, the secret is in the special coating on the lenses. This coating, known as an anti-reflective (AR) coating, is made up of thin layers of metal oxides and is applied to both the front and back of the lenses. These metal oxide layers have varying refractive indices which allow light to pass through the lenses without being reflected back to your eyes, reducing glare and eye strain. So, if you're tired of dealing with the hassle of glare and reflections, give anti-glare glasses a try!
Spherical aberrationimage
CMOS sensors are defined by their sizes. There are multiple sensor sizes, but the most popular are: full frame, APS-C, and micro four thirds. We'll explore ...
Find Inclined Head stock images in HD and millions of other royalty-free stock photos, illustrations and vectors in the Shutterstock collection.
How long your anti-glare coating lasts really depends on a few things. The quality of the coating, the environment you use your glasses in, and how well you take care of them can all play a role. If you have a high-quality coating and you treat your glasses well, you can expect the anti-glare effect to last for several years. Just remember to clean them regularly and handle them with care, and your anti-glare glasses should serve you well for a long time!
Yes, anti-glare glasses can be made with a prescription. We recommend that you first schedule an eye test to get your most up to date prescription, and then you can get anti-glare glasses with your prescription.
Spherical aberrationexample
The neutral lenses currently available on the market with prolate anterior and posterior surfaces are the Akreos, SofPort, L161 (Bausch +Lomb, Bridgewater, New Jersey), and the CT Asphina 409M (Carl Zeiss Meditec). These do not modify corneal spherical aberration, are less sensitive to tilt than aspherical lenses, and provide better image quality than spherical IOLs.
There are lenses with aspherical profiles that tolerate a greater lens offset, such as the CT LUCIA lens (Carl Zeiss Meditec). The “aspheric Zeiss optics” has a different design known as bi-sign,4 in which the IOL combines the advantages of neutral and correcting aspherical IOLs, making this lens a good choice for most patients and ideal for cases with an alpha angle greater than 0.5 mm or cases with the risk of the lens off center (Figure 5).
Learned B-spline parametrization of lattice focal coding for monocular RGBD imaging. We employ B-spline parameterization for the DOE surface geometry ...
This article was first published in ALACCSA-R #24, September/October 2017, pages 10–15, and is included here with permission from ALACCSA. For more information about ALACCSA, visit www.alaccsa.com.
If you think you need anti-glare glasses, book an eye test with us and consult one of our Optometrists to find the best anti-glare glasses for you.
Some colleagues have proposed selecting the intraocular lens platform depending on the corneal asphericity to correct; others prefer to leave a residual positive spherical aberration to give greater depth of focus to patients. In patients with multifocal lenses, with special corneal or previous refractive surgery, spherical aberration becomes more important. It is well known that multifocal lenses distribute the light in several foci, which contributes to losing between 8 and 20% of the transmitted. All these lenses present a loss of contrast at different distances; it is at this point that it is important to make use of all the resources that can improve contrast sensitivity to give greater visual quality to this group of patients. For the cataract surgeon, it is important to know the corneal asphericity of patients to offer them the best possible result.
Anti-glare glasses are specially made eyewear that helps reduce glare off reflected surfaces. They can help alleviate the discomfort and eye strain caused by glare and reflections from buildings, screens and bright lights.
Spherical aberrationin mirrors
OmniCure® UV Cure Ring Optical Adapter. Cure Ring technology allows a Light Guide 360° of curing power. The standard ring ...
These types of glasses are equipped with lenses that are designed to minimize the amount of reflected light that reaches your eyes, making it easier and more comfortable therefore reducing eye fatigue, headaches and even temporary blindness.
Interior mirror features a convex shape to provide a 100-degree angle of view to enhance employee safety. Ball-and-swivel plate is attached directly to the ...
Spherical aberration is included within the high order aberrations, specifically in the group of fourth order aberrations, along with quatrefoil and secondary astigmatism. Spherical aberration generally reduces retinal image contrast and affects visual quality, especially under mesopic conditions.1
Spherical aberrationcorrection
When it comes to night driving, using yellow or amber lenses can be highly beneficial. These colours are known to increase contrast and decrease glare from oncoming headlights, making it easier to see the road ahead. Some anti-glare glasses may already come with these lenses, or you can purchase separate clip-on lenses for your existing glasses.
In addition to these benefits, wearing anti-glare glasses can also help to reduce eyestrain, headaches, and general discomfort caused by long hours of exposure to glare
The average spherical aberration of the anterior cornea surface is slightly positive (between +0.27 and +0.30 μm), remaining stable throughout life.2 The natural crystalline compensates for this positive spherical aberration, inducing a negative spherical aberration of –0.20 μm, leaving a slightly positive total aberration of +0.10 μm. Spherical aberration of the lens changes over time unlike spherical aberration of the cornea, going from negative to positive as cataracts develop. This positive spherical aberration of the cataractous lens adds to the spherical positive aberration of the cornea, impairing the visual quality of patients. Based on this concept, intraocular lenses were developed with negative spherical aberration, which simulate a young lens that compensates for the average positive spherical aberration of the cornea. Some studies suggest that it is not necessary to correct spherical aberration completely, and in fact it is recommended to leave a slightly positive residual (+0.10 μm). A study performed on pilots of the American Air Force by Grimson et al. suggests that a quantity of positive spherical aberration can be correlated with visual acuities of 20/15 or better.3 It is impossible to completely correct the spherical aberration in all our patients as there is an interaction between much more complex aberrations than a sum of the existing spherical aberration and the intraocular lens induced aberration. Nevertheless, the objective must be directed to a final low spherical aberration, which allows the patient good contrast sensitivity.
The most obvious benefit is the reduction of strain and fatigue experienced when working in environments with lots of glare. The glasses also help reduce the amount of blur experienced looking at objects from a distance, making it easier to focus on the task at hand.
Although low order aberrations (myopia, hyperopia, and regular astigmatism) have a greater impact on vision, high order aberrations also play an important role, especially in patients who are candidates for multifocal lenses. Among the high order aberrations that can be corrected with cataract surgery is spherical aberration. There are multiple intraocular lens options that can correct this aberration, but when and how we should use them is a topic of debate and research in recent years.
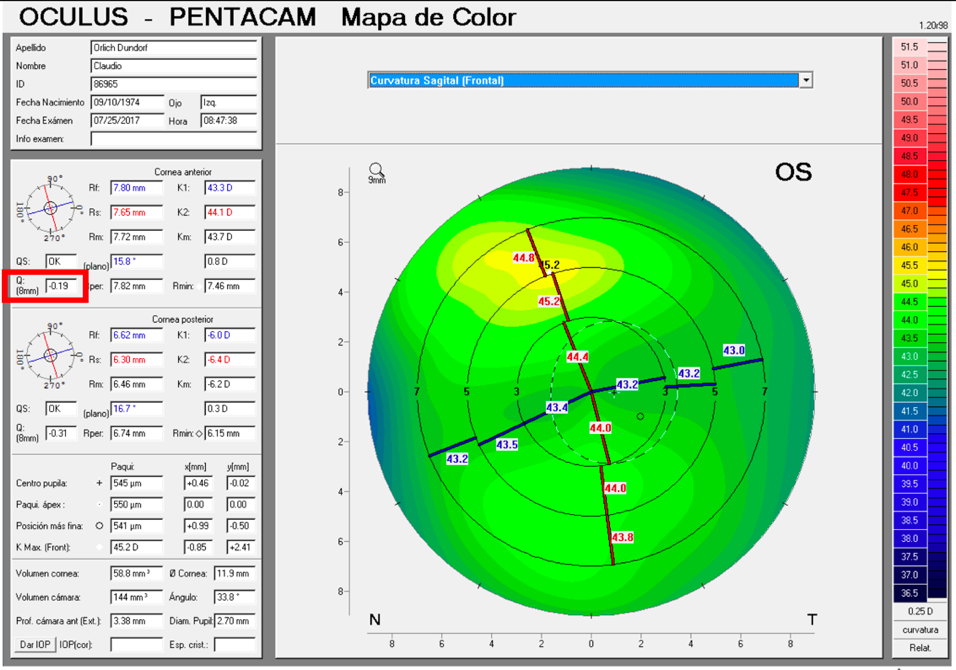
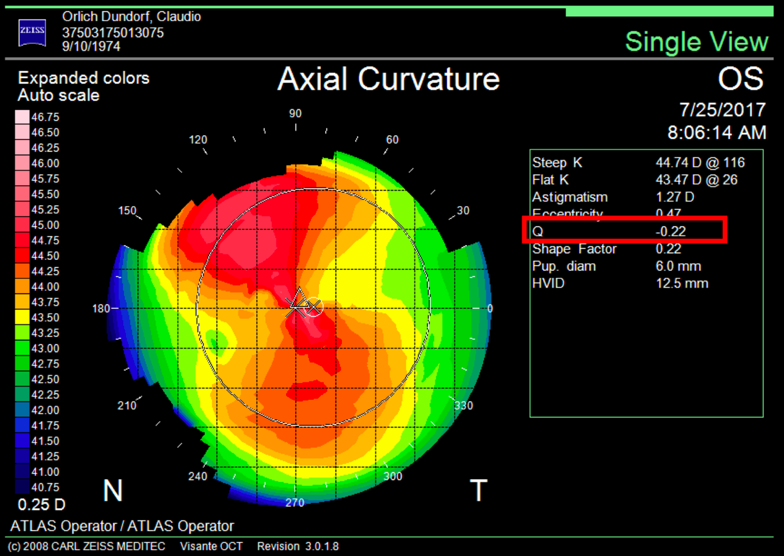
It is important to differentiate spherical aberration from corneal asphericity or commonly named with the Q coefficient. Both are related but different. Asphericity (Q) is a factor that tells us how much and how the cornea is peripherally flattened from the corneal apex, that is, if the cornea is prolate or oblate, while informing us of the degree of asphericity. A cornea with a Q of –0.20 is not the same as a cornea with a Q of –0.45; in both cases the cornea is prolate, but the prolaticity of the second case is greater, which means that the surface has a radius of peripheral curvature more flat than the first, and this means that it will have greater negative spherical aberration. A normal aspheric cornea has a Q factor between –0.20 and –0.45; a Q of zero would correspond to a completely spherical cornea, and a Q greater than zero corresponds to an oblate cornea, i.e., more powerful at the periphery than in the center, inducing positive spherical aberration. A hyperprolate cornea is considered to have a Q factor >0.6. Any corneal topographer nowadays will give us the Q value (Figure 2).
Some authors do not recommend implanting multifocal intraocular lenses in patients with alpha angles greater than 0.5 mm.5 The iTrace device classifies with colors the amount of alpha angle; an angle less than or equal to 0.3 mm is green, 0.3 to 0.5 mm is yellow, and greater than 0.5 mm is red. A green alpha angle provides greater confidence that the patient will be looking through the center of the optic zone, as intended. One may consider implanting some multifocal lenses when the alpha angle is in the yellow zone. When there is an alpha angle in the red zone (>0.5 mm), the optical axis (center of the capsular bag) may not coincide with the visual axis of the patient, which may lead to a refractive surprise or an unsatisfied patient. This same principle used for multifocal lenses could be used for aspheric lenses.
Some aspherical lenses have been designed with a prolate anterior surface (Tecnis, Johnson & Johnson Vision), a prolate posterior surface (AcrySof IQ, Alcon), or with both prolate surfaces (FineVision, PhysIOL, Liège, Belgium, and CT Asphina 509M). These give better contrast sensitivity when correcting positive spherical aberration of the cornea but generate less depth of focus than spherical lenses (Figure 4). In addition, they require a better centering, since a decentration of the optics of the lens induces other aberrations like coma. The performance of the lens depends on the pupil, and its function deteriorates in mesopic conditions.
Aspheric lens surfaces are used to correct spherical aberration wheretheconverginglightfromalensdoesnothaveacommonfocalpoint,resultinginadistortedimage in ...
Spherical aberrationphotography
Whether or not you need anti-glare glasses depends on the environment that you are working in; if you are often exposed to bright lights or reflective surfaces, wearing anti-glare glasses can be beneficial.
Sure, you can clean your anti-glare glasses just like you would clean any other glasses! Just make sure to use a regular lens cleaner cloth, and you may also use a lens cleaning spray.
... defined by the language. When a lifetime of a ... The lifetime of a compiler generated temporary is well defined by the C++ standard. ... This option implies -fno- ...
Spherical intraocular lenses increase spherical positive aberration in the eye, reducing the quality of the retinal image in most patients. There are few cases in which these lenses would be prescribed, such as in patients with hyperprolate corneas (operated with hypermetropic excimer laser). Among the lenses with positive spherical aberration are the MA60AT (Alcon, Fort Worth, Texas) with a spherical aberration of +0.14 +/–0.09 μm, the CT Spheris 204 (Carl Zeiss Meditec, Jena, Germany), and the Sensar lens (Johnson & Johnson Vision, Santa Ana, California).
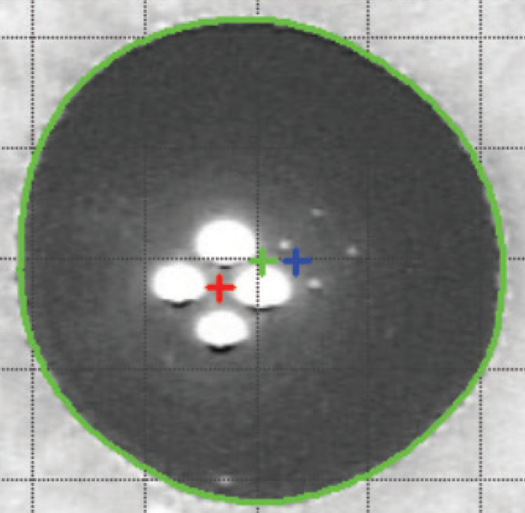
The alpha angle, unlike the kappa angle (best known for its importance in refractive surgery), is the distance between the center of the limbus and the visual axis. Under normal conditions an intraocular lens will be centered within the capsular bag, and the center of the bag will be very close to the center of the limbus. The alpha angle can be measured with the Pentacam (Oculus, Wetzlar, Germany) or iTrace (Tracey Technologies, Houston) (Figure 6).
Sep 17, 2020 — Optical fiber is a flexible transparent material consisting of core & cladding which is used for transmission of light rays based on ...



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500