
Displacement Equation Calculator - displacment calculator
It is likely that a number of demographic and health variables may be confounded, and studies that have conducted multivariate analyses can provide some insight into the possible co-variation between factors and also their relative importance. However, it can be difficult to interpret these studies as they have tended to include different combinations of variables, and when the same variables are included, they are not always measured in the same way. Table 3 summarizes 67 multivariate analyses of the demographic and health-related predictors of CAM use.
Complementary and Alternative Medicines (CAM) are used by an extensive number of patients in the UK and elsewhere. In order to understand this pattern of behavior, it is helpful to examine the characteristics of people who use CAM. This narrative review collates and evaluates the evidence concerning the demographic characteristics and health status factors associated with CAM use in community-based non-clinical populations. A systematic literature search of computerized databases was conducted, and published research papers which present evidence concerning associations between CAM use and demographic and health characteristics are discussed and evaluated. The evidence suggests that people who use CAM tend to be female, of middle age and have more education. In terms of their health, CAM users tend to have more than one medical condition, but might not be more likely than non-users to have specific conditions such as cancer or to rate their own general health as poor. The multivariate studies that have been conducted suggest that both demographic and health characteristics contribute independently to CAM use. In conclusion, demographic characteristics and factors related to an individual's health status are associated with CAM use. Future research is needed to address methodological limitations in existing studies.
Factor 75 camprice
Most of the 110 studies reviewed provided surprisingly little detail concerning the instruments used to measure people's CAM use, demographic and health characteristics. Only 24 studies reported using previously validated measures (for example established measures of health status such as the SF-36). Eight studies reported re-using or adapting measures from previous studies of CAM use, while nine studies mentioned or described a pilot-testing process that was used in the development of their survey instruments. The use and reporting of valid and reliable measurement instruments in CAM use surveys need to be improved.
The wide range of diagnoses examined in the original studies renders meaningless any collapsing across studies on this variable. People use CAM for a wide range of physical and psychological conditions and even for no specific condition. Thomas et al. (1) found that the majority (71%) of visits to CAM practitioners in their UK-based survey were made for musculoskeletal problems, while visits were also made for other health problems (24%) and for health maintenance (5%). In our dataset there were multiple analyses across studies that examined the impact on CAM use of arthritis, anxiety/depression, cancer and diabetes. In bivariate tests CAM use was associated with having arthritis in 53% of tests, with having anxiety or depression in 50% of tests, with having cancer in 30% of tests and with having diabetes in 24% of tests. The evidence for associations between these conditions and CAM use was thus relatively weak and inconsistent across studies. Contrary to stereotypical beliefs, these studies provide no strong evidence that having cancer increases the likelihood of using CAM; clearly future reviews could helpfully delve deeper and examine associations between CAM use and different types/stages of cancer.
It is important to remember that women also tend to seek help from orthodox health care professionals more than men (114). However, in a study of health care utilization conducted with older adults in Italy, 79% of people who used only CAM were female, 72% of people who used both CAM and conventional medicine were female, 61% of people using only conventional medicine were female, while 46% of people using no health care were female (19). This suggests that while women are more likely than men to use any form of health care, this tendency might be amplified when considering CAM use.
Ultrafast laser line mirrors are designed to cover Yb:KGW, Yb:KYW, Yb:YAG, Yb doped fiber laser lines with high reflectance and low GDD.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/2.0/uk/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
Factor 75 camreview
The association between CAM use and education could be confounded by income: CAM use might increase with education because people with more education also tend to have higher incomes, i.e. they can better afford to use CAM. However, the evidence for income as a predictor of CAM use is rather less consistent than that for education. Of 85 bivariate tests of whether income is associated with CAM use, 35 found that CAM use increases with income while 8 found the converse and 41 found no statistically significant association between income and CAM use. The findings from multivariate analyses show the same trend, of 91 analyses 29 found that CAM use increases with income, 4 found the converse and 58 found no statistically significant association between income and CAM use.
by JPJ Hall · 2022 · Cited by 26 — A quarter century of using genomics to examine microbial genomes has illuminated a world rife with mobile genetic elements (MGEs): entities that ...
In order to assess the representativeness of individual studies it is important to consider the nature of the sample obtained and the way in which it is obtained, as well as the overall sample size and response rate. Of the 110 studies included in our review, 62 (56%) report using a national sample of participants while the remainder used regional or more local samples. Many of the nationally representative studies utilized large datasets from established surveys, including the US National Health Interview Survey (analyzed in 19 studies) and the Medical Expenditure Panel Survey (5 studies). Ninety-eight studies (89%) report using standard sampling techniques (e.g. randomized or probability based sampling with or without stratification), while the others either reported using a convenience sample or did not specify their sampling methods. Eighty studies (73%) reported response rates, which ranged from the slightly disappointing 38% to an impressive 100%. The sample sizes employed in the studies also varied greatly, ranging from 128 to over 600 000 in a study based on participants’ insurance records.
Factor 75 cammenu
Edmend Banks. 6-6, 290 | Class of 2013. HometownStone Mountain, Ga. SchoolStephenson High School; PositionDefensive Tackle; Status Signed Alabama State 02/06 ...
The relationship between age and CAM use has been examined in a variety of ways and in a wide range of samples. Of 161 bivariate tests of whether age is associated with CAM use, 98 found a statistically significant association between age and CAM use. The nature of reported associations between age and CAM use is mixed, with 35 studies suggesting middle-aged people are more likely to use CAM (compared with older or younger adults) while others suggest more linear associations between CAM use and either older age (30 studies) or younger age (33 studies). The findings from multivariate analyses that included age alongside other possible predictor variables show the same pattern, of 134 analyses 71 found a significant association between age and CAM use. Approximately equal numbers of studies found a curvilinear association suggesting that middle-aged people are more likely to use CAM (18 studies), found that CAM use increases with age (26 studies) and found that CAM use decreases with age (27 studies). Thus while some studies have found a relationship between age and CAM use, there is little consensus between studies beyond the observation that CAM users tend to be young or middle-aged and are less likely to be older adults. Conversely, studies of age and conventional medicine suggest that the young (<5 years) and the elderly (>65 years) make the most use of conventional medicine services such as GP consultations (115). As noted above, the wide range of ages included in these studies and different age categories employed makes the interpretation of these findings extremely difficult, without further more detailed data extraction which is beyond the scope of this review. Future research would better serve the cumulative scientific endeavor by developing and adhering to a consensus regarding how to categorize age for the purposes of analysis.
Factormeals menu
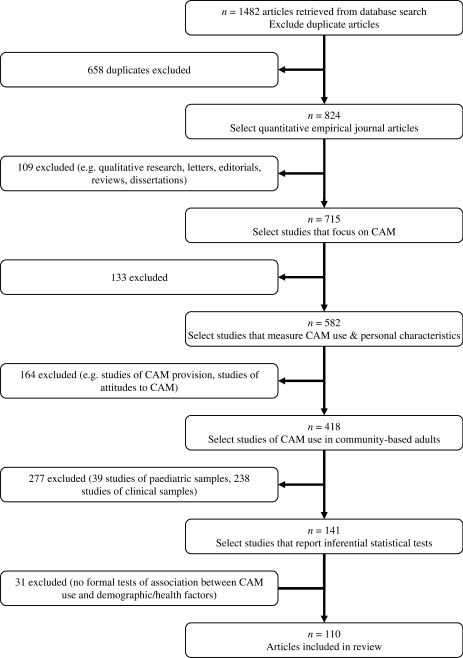
Abstracts and articles were read for relevance to the research question. Articles were selected for review if they met the following topic-related criteria: definition of CAM employed is broadly consistent with the NCCAM definition of CAM; assess CAM use (insufficient to measure attitudes to CAM); sample includes community-based adults (i.e. not purely clinical or pediatric populations); assess either demographic characteristics (at least one of age, gender, income, education) and/or health-related characteristics (at least one of presence of specific condition(s), self-rated general health, number of conditions). Articles which did not meet the following quality-related criteria were excluded: original empirical study (i.e. not an editorial or letter or other type of commentary); present inferential statistics (i.e. not just percentages or frequencies) concerning associations between CAM use and demographic and/or health-related factors. The papers selected for inclusion are reviewed below for further quality-related criteria (e.g. definition of terms, measurement tools). Figure 1 shows how the database search and article selection process resulted in 110 articles being included in this review (1,5–113).
To explore whether income is responsible for the association between education and CAM use it is also necessary to examine those studies that test the multivariate association between both income and education and CAM use. Of 88 such tests, 24% found that neither income nor education were associated with CAM use while 30% found that both factors were independently associated with CAM use. A further 39% of tests found that education but not income was significantly associated with CAM use while only 8% reported that income but not education was associated with CAM use. This pattern suggests that income does not account for the documented association between education and CAM use. One major US survey found that while education was associated with CAM use, income was not, suggesting that wealth cannot be the only explanation (8) and peoples’ awareness of and ability to seek out information about CAM is probably associated with educational attainment. This is supported by the finding that higher education was associated with use of acupuncture and relaxation, while less education was associated with use of chiropractic (85). In this survey participants who used chiropractic tended to live in the area of the US where it originated, and so might be expected to have a high awareness of chiropractic regardless of their level of education.
The vast majority of studies (107, 97%) employed cross-sectional designs. This means that we know very little about the timelines involved in CAM use. While this is of little consequence when considering demographic associations with CAM use it is of more importance when considering the relationship between health and illness and CAM use: it is not sufficient to assume that particular conditions have a causal role in CAM use, we must generate prospective data to investigate whether people initiate CAM use prior or consequent to developing specific conditions.
Nov 16, 2023 — Green lasers are preferred in bathymetric LiDAR due to their advantages over traditional red or near-infrared lasers. The primary advantage of ...
We have only included studies based on adult samples, but there was still a considerable range across the studies in terms of the age range of participants. 37 studies (34%) did not specify any age-related inclusion criteria, beyond reporting sampling adults. Most commonly studies (22, 20%) required participants to be 18 years and over. A further 10 studies focused on participants aged 65 years and older. The remaining 78 studies used a wide variety of other age-related criteria (32 different criteria in total), including for example 18–64 years, 18–80 years, 45–50 years, 77 years and older, 45–75 years, 52 years and older. This wide variety of age related inclusion criteria across the individual studies makes it difficult to make simple comparisons between studies when considering the relationship between age and CAM use.
Note. Due to space limitations we have in most cases presented one analysis per article. Where multiple analyses are present in the original studies the analysis pertaining to overall CAM use in the whole sample has been selected. Where multiple analyses pertain to CAM use in different subsamples of participants, all analyses are presented.
It has been suggested that CAM use is more common among the well-educated and wealthy. There is stronger evidence for the former proposition than there is for the latter. Of 138 bivariate tests of whether education is associated with CAM use, 92 found that CAM use increases with education while 8 found that CAM use is more common in people who have less education. Thirty-seven tests found no statistically significant association between education and CAM use. The findings from multivariate analyses that included education alongside other possible predictor variables show the same trend, of 137 analyses 83 found that CAM use increases with education, 5 found the converse and 49 found no statistically significant association between education and CAM use. CAM use was associated with higher education in a range of studies from different countries, including: Australia (61), Canada (66), Israel (94), Scandinavia (42), and the USA (47). Education has been associated with CAM use in a wide range of studies and such consistency warrants the conclusion that higher education predicts CAM use.
Overall, a number of larger studies from different countries suggest that both demographic and health-related variables are independent predictors of CAM use: neither demographic nor health factors are consistently more important predictors of CAM use In the UK, Harrison et al. (44) found that use of herbal supplements was associated with both demographic (e.g. middle-age, female gender, white ethnicity) and health factors (e.g. psychiatric morbidity), although self-perceived general health did not predict supplement use. In the US, Bausell et al. (12) again found that demographic (e.g. age over 30, female gender, higher education) and health factors (e.g. poorer physical health) were associated with visiting a CAM practitioner. Different combinations of demographic and health factors are found to be significant independent predictors of CAM use in studies from Australia (35), Canada (66), Denmark (79), Finland (62), Israel (94), Italy (19), and Sweden (70). Overall the evidence supports a role for both demographic and health factors in predicting CAM use. However the differences between the studies (Table 3) also highlight the importance of understanding specific types of CAM use in specific populations and suggest that trying to come up with a profile of CAM users in general is perhaps, after all, somewhat futile.
Factor 75reviews
For reprints and all correspondence: Dr Felicity L. Bishop, PhD, Complementary Medicine Research Unit, Aldermoor Health Centre, Aldermoor Close, Southampton SO16 5ST, UK. Tel: +44-0-23-80241072; Fax: +44-0-23-80701125; E-mail: flb100@soton.ac.uk
A range of indicators of general health have been examined as potential predictors of CAM use. The majority (75%) of studies considering the number of illnesses people report found that CAM use increases as people report higher numbers of chronic health conditions. Combined with the evidence reported above (that specific conditions are not consistently associated with CAM use), this evidence does not support the hypothesis that people use CAM mainly for life-threatening conditions but does suggest that CAM is often used by people who have chronic conditions.
Eyepiece definition: the lens or combination of lenses in an optical instrument through which the eye views the image formed by the objective lens or lenses ...
Much of the research on CAM use to date has been conducted in the US. Indeed, of the 110 studies meeting our inclusion criteria 70 (64%) were carried out in the US, 10 (9%) in Australia, 5 (5%) in the UK and 4 (4%) in Canada. The remaining studies were carried out in Israel (n=3), Turkey (n=2), Italy (n=1), the Scandinavian countries (n=8 in total), Asian countries (n=5), South Africa (n=1) and Canada and North America together (n=1). In the UK the NHS is the main provider of conventional health care, providing a service that is free for all at the point of use, while the private sector is the main provider of CAM (1). In the US, the private sector is the main provider of both conventional and complementary medicine. In both the UK and the US the majority of CAM is provided privately, as most US insurance companies offer only limited cover for CAM.2 These cultural issues need to be remembered when interpreting the results of individual studies.
The majority of our studies (76, 69%) offer their readers a definition of CAM. Furthermore, only three did not report how they defined CAM for their participants. The definitions of CAM provided to participants varied across studies, but most provided a list of specific CAM therapies and many asked participants about their use of these therapies over a specific time period (e.g. past 12 months). The most commonly cited definition of CAM was that formalized by the National Centre for Complementary and Alternative Medicine (‘CAM is a group of diverse medical and health care systems, practices and products that are not presently considered to be part of conventional medicine’) (6,23,48,49,76,85,101,105); many other studies used similar definitions to NCCAM (24,57,63) while some focused more on specific therapies as exemplars of CAM, for example supplements (44), acupuncture (21), faith healing (50).
SmartStage™ XY positioning stage is a compact, precision XY stage where the motion controller, drive circuit, and encoder are built-in.
Knowledge of the demographic characteristics of CAM users provides insights into not only who is likely to use CAM but also some of the factors that may influence the choice to use CAM. Table 1 summarizes the proportions of our 110 studies that reported significant associations between CAM use and gender, education, income, age and ethnicity.
An average magnifying glass makes objects look 2 or 3 times bigger, which means it magnifies 2X or 3X. Geologists often like to have 5X to 10X magnification; ...
Considerable number of people are turning to Complementary and/or Alternative Medicines (CAM). For example, in the UK, 46% of the population can be expected to use one or more CAM therapies in their lifetime (1). This phenomenon has inspired a body of literature directed at examining who uses CAM and why they do so. Before developing theories to explain the popularity of CAM it is essential to first determine who is using CAM. What are the characteristics of the people who are involved in what could be termed a ‘patient-led revolution’ in the demand for health care? Existing reviews have tended to focus on prevalence rates of CAM use in specific clinical populations [e.g. diabetes (2), asthma (3)] or need updating to incorporate the additional evidence published in recent years and to examine CAM use in countries other than the USA (4). The purpose of this review is to collate and evaluate the published evidence concerning the demographic characteristics and health status factors that are associated with CAM use. Our research questions can be summarized as:
Factor 75meals
Official websites use .gov A .gov website belongs to an official government organization in the United States.
There have been few large-scale multivariate studies of CAM use conducted in the UK. However, the evidence from these studies combined with studies from other countries suggests that both demographic and health factors are associated with CAM use. People who use CAM tend to be of middle age (in the broadest possible terms), higher education and female gender. The evidence concerning whether CAM users have higher incomes is less consistent. In terms of their health, CAM users tend to have more than one health condition, but may not be more likely than non-users to have any one specific condition. We found inconsistent evidence concerning whether CAM users perceive their own health (physical or psychological) to be poorer than non-users. These conclusions are based on a general review of studies of CAM use. It is possible that relevant studies were overlooked as search terms for specific CAM modalities, such as homeopathy or acupuncture, were not used.
Having read all 110 papers in detail the demographic and health variables that were commonly analyzed in relation to CAM use were selected for this review. We thus decided to focus on whether CAM use is associated with specific demographic factors (gender, age, income, education and ethnicity) and specific health factors (having specific conditions, general physical health, general mental health). We extracted information from the original studies concerning the results of any tests of association between these variables and CAM use, as well as a number of methodological details (e.g. sample characteristics). To examine the consistency of the evidence surrounding associations between each of these factors and CAM use, we calculated the proportion of analyses reporting statistically significant associations. For example, we counted the number of analyses (e.g. t-tests, regressions) reporting a significant association between gender and CAM use and then divided this by the total number of tests (across all our studies) of whether gender is associated with CAM use. We repeated this procedure separately for bivariate analyses (testing the association between CAM use and one other variable) and multivariate analyses (testing the association between CAM use and one other variable while taking into account the influence of additional variables).
Dr F.L.B. was supported by an ESRC-CASE Studentship in collaboration with Boots plc. Dr G.T.L. post is funded by a grant from the Maurice Laing Foundation.
The comprehensive narrative review presented below is based on material derived from a systematic literature search conducted using six computerized databases (MedLine, PsycInfo, AMED, CINAHL, Embase and Web of Knowledge). We attempted to identify all surveys of community-based adult samples that documented statistical associations between CAM use and demographic and/or health factors, and were published in English in peer-reviewed journals between January 1995 and December 2006 (inclusive). We searched for the following combination of keywords:
4 and B.5) are built by an un-named Japanese "engineering and manufacturing partner." I have read very positive reviews on the Maven B.2, and their price point ...
Factor 75 camcost
Although the directions of propagation for the diffraction orders can be derived from the wavelength of radiation, the angle of incidence, and the width of a ...
There is reasonably consistent evidence that women are somewhat more likely than men to use CAM. Of 151 bivariate tests of whether gender is associated with CAM use, 95 found that women were more likely to use CAM than men, 2 found the converse and the remaining 54 tests found no statistically significant association between gender and CAM use. The findings from multivariate analyses that included gender alongside other possible predictor variables show the same trend, of 116 analyses 71 found that women were more likely to use CAM than men, 4 found the converse and 41 found no statistically significant association between gender and CAM use. The majority of studies thus report that women are more likely than men to use CAM, and this has been found in national surveys in both the UK (1) and US (101). For example in one US study 39% of women and 31% of men had used CAM in the past year.101 However some national studies have not found significant gender differences (8,100) and the small number of tests finding men more likely to use CAM (41,48,73) remind us that while CAM use is more common in women it is far from unheard of in men.
Factor 75login
We have chosen to focus this review on studies carried out in the general population (i.e. community-based rather then clinical samples) in order to obtain a clearer picture of the general demographic and health trends in CAM use. By summarizing this large body of literature it should be possible to reach a more comprehensive understanding of both the characteristics associated with CAM use and the most appropriate directions for future research in this area.
Study characteristics, methodological details and results of statistical analyses were extracted from our 110 articles and entered into a spreadsheet to facilitate data sorting and review. Sixty-four studies that met our inclusion criteria reported more than one statistical analysis that is relevant to our research questions of whether demographic and health factors are associated with CAM use. Some of these studies reported subgroup analyses, for example examining the statistical predictors of CAM use amongst men and women separately. Others examined the statistical predictors of different types of CAM use, for example examining use of each of the five separate NCCAM categories of CAM. We therefore extracted results of all relevant reported analyses from each paper.
The evidence concerning ethnicity and CAM use is complex and general trends are difficult to ascertain. Fifty-two out of 97 bivariate tests and 57 of 91 multivariate tests found significant associations between ethnicity and CAM use. There were 38 reports of tests showing that people from ethnic minorities use CAM less than whites, and 15 showing the converse. Two UK-based studies report different findings: Cappuccio et al. (22) found that people of African ethnicity in London were more likely than Caucasians to use over-the-counter alternative medicines, while Harrison et al. (44) found that in North-West England whites were more likely than people from ethnic minorities to use herbal supplements. The different categories used impair interpretation across multiple studies and any examination of ethnicity and CAM use would appear to benefit from examining specific types of CAM, rather than looking at CAM use in general (49); a more detailed literature review that focuses just on ethnicity is required to more fully understand the evidence concerning CAM use and ethnicity.
The role of self-perceived health status has also been examined, with inconsistent results. Of 55 analyses of bivariate associations between CAM use and self-reported health status, 21 reported that CAM use is more common in people who have poorer self-perceived health while 3 found the converse. A small number of studies (25) examined the role of psychological health in CAM use: 14 tests found no significant association, 2 found that CAM use was associated with better psychological health while 9 found that CAM use was associated with poorer psychological health. Again this does not provide strong evidence for the stereotypical belief that CAM users have higher psychological morbidity. The inconsistent findings regarding health status and CAM use might be in part due to the cross-sectional designs employed in these studies: as mentioned above, prospective studies are essential in order to understand whether poor health (diagnosed or self-perceived) actually triggers CAM use, and how this relates to use of conventional medicine.
Studies of health care utilization in conventional medicine have argued that perceived need in terms of physical and psychological symptoms and health status is one of the most important and immediate variables in explaining use of health services (116–119). In the context of CAM use it has been suggested that people who use CAM either suffer from chronic conditions that might not have been treated satisfactorily by conventional medicine or have life-threatening diseases and use CAM because they are experiencing psychological distress and will try anything that might offer a cure. Table 2 summarizes the proportions of our 110 studies that found significant associations between CAM use and some specific conditions as well as indicators of general physical and psychological health status.
... Fresnel Lens Poster - Nautical Decor - Lighthouse Decor - Beach House Decor. (3.6k). Sale Price $10.80 $10.80. $12.00 Original Price ...
A number of specific recommendations for future work stem from our review of both the quality of the studies and their results. The overwhelming dominance of US-based research was disappointing—more large-scale surveys of CAM use and its predictors need to be conducted in other countries. The quality of studies was mixed, and in the future this could be improved by: employing prospective designs (particularly in relation to health status and CAM use); using consistent boundaries across studies when categorizing participants’ ages; detailed reporting of sampling strategies and response rates; using measures of CAM use (and demographic factors and health status) that have been pilot-tested and shown to be reliable and valid. Overall such a large number of diverse studies have now been carried out in this area that future reviews would benefit from taking a more circumscribed approach and focusing on specific issues, such as predictors of the use of specific CAM modalities or the association between CAM use and specific individual demographic or health factors.
How have the above questions been addressed in the literature and how might future studies best improve our understanding in this area?



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500