
Cooper Vision Contact Lens - lens vision
In short, a 0 km or -1km (above the surface of the earth) depth earthquake is physically impossible, since earthquakes always occur due to two blocks or rocks of crust slipping past one another, which is impossible on the Earth’s surface.
The number of focal points produced by a diffractive lens depends on the specific details of photonic engineering, including the number of concentric rings and the pattern of their spacing. As more focal points are added to a diffractive lens, combined with a refractive lens, the difference between the focal points becomes indistinguishable to the eye, producing an apparent continuous gradient of focus on the retina. Despite precision of design and fabrication, benefits may be limited by unwanted optical effects due to sharp edges.
In general, shallow earthquakes tend to be more damaging than deeper ones, since seismic waves from deep earthquakes travel farther to the surface, losing energy along the way. The strength of an earthquake shaking at the surface that occurs at 400 kilometers deep is noticeably less than if an earthquake occurred at 10 kilometers depth. Moreover, shallow-focus earthquakes often produce much more aftershocks than deep-focus earthquakes.
CTFmeaning Education
Most multifocal IOL designs, such as bi- and trifocal IOLs, generate multiple foci on the retina to capture the necessary clarity of vision for multiple focal distances. In these types of lens implants, IOL centration assumes critical importance since a decentered IOL, relative to the visual axis, may induce high-order aberrations and decrease post-operative visual function due to “looking through” diffractive rings of the IOL instead of the central optical zone as intended [26]. Thus, decentration could directly lead to a negative impact on the visual outcomes. Additionally, as a result of the distinct foci with different properties in the IOL, severe changes near the transition points could have a negative impact on the patient’s vision, as optical distortions are likely to take place. Alternatively, pupil diameter may also influence the ratio between distance and near additive power provided by the IOL. It has been previously described that patients with a small pupillary diameter (below 3.0 mm) are not good candidates for the traditional asymmetric refractive multifocal IOL, especially the Lentis Mplus Toric (Oculentis GmbH, Berlin, Germany) [26]. Also, patients with a large pupil are considered at increased risk for glare dysfunction, and may experience optical aberrations, diffraction, and photic phenomena such as glare, starbursts, and halos around light sources [27, 28]. A recent study comparing through-focus vision performance and light disturbances of FineVision (PhysIOL, Liège, Belgium) and PanOptix (Alcon Laboratories, Fort Worth, TX, USA) trifocal IOLs to the Symfony extended depth of focus IOL was published by Escandón-García and colleagues in Portugal [29]. They found that the trifocal IOLs grant better performance at near distance while extended depth of focus IOLs performed better at intermediate distance. Additionally, objective dysphotopsia was not reduced in extended depth of focus IOLs as compared to the trifocal IOLs [29].
Earthquakes and tsunamis are natural disasters that are sometimes closely connected through a cause-and-effect relationship.
In April 2017, Precizon Presbyopic IOL (Ophtec BV, Groningen, Netherlands) favorably concluded clinical trials (Clinical Trial NCT02409771) and results were presented at the 2017 European Society of Cataract and Refractive Surgeons meeting [32]. The prospective, multicenter European trial included 60 patients scheduled for cataract or refractive lens exchange surgery with a follow-up of 3 months. Investigators reported good uncorrected visual acuity at near, intermediate and distance and 80% of patients achieved spectacle independence, with an additional 18% requiring occasional spectacle use. The majority of patients did not report issues with halos and glare, however approximately one-third of patients did report little to moderate disturbance. The lens delivered a concept of an IOL more tolerant to pupil size and dislocation, receiving its CE marking in May 2017. Additionally, in September 2017, Swiss Advanced Vision launched EDEN, an IOL that uses the Instant Focus EDOF (extended-depth-of-focus) technology that offers continuous vision with minimized dysphotopsia, while preserving resolution and contrast sensitivity.
The first multifocal IOL was developed by Precision-Cosmet (Buffalo, NY, USA), later transferred to IOLAB Corporation (CA, USA) and finally Bausch & Lomb (Rochester, NY, USA), who marketed the lens as NuVue. The novel design of NuVue facilitated two focal points [6]. Multiple focal points were created by combining two radii in a single lens in a bullseye pattern, where the center of the bullseye had one power (power A), the first ring had a second power (power B), the next ring power A, then B, and so on. The result is two focal points simultaneously present in the eye: one for distance viewing and another for near. The relative contribution of each focus is modulated by the pupil diameter under bright and dark lighting conditions. Other similarly designed lenses were soon developed, with more than two focal points, including the TrueVista 68STUV, from Storz, with three focal points [6, 7].
Ctfstands for in computer
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
CTF lenses can provide focus within the entire depth of field, meaning that the image more closely mimics the visual experience of the natural lens. Because the focal points are not limited to one or two discrete locations, but graduated over a larger area, some alignment issues are reduced, making placement of the lens “more forgiving” and less sensitive to pupil size.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
What doesCTFmean in cyber security
This brief review describes the evolution of currently available IOLs to address presbyopia, and a look toward new technologies, such as continuous transition focus (CTF) lenses, is highlighted. This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Accurate determination of earthquake depth is necessary for assessing seismic hazards, discriminating earthquakes from nuclear explosions, interpreting Earth’s structure, and understanding tectonic processes. Even though it has long been believed that earthquakes cannot occur at a depth of more than 700 kilometers, new proof of it gives us an alternative explanation that those deep earthquakes are caused by some kind of "phase transition", where the physical structure of the rocks suddenly changes to a different state – a process still waiting to be explored and researched.
The methods used to determine the depth of an earthquake vary depending on where an earthquake occurred relative to seismic stations.
The vast majority of earthquakes are shallow. Of the 56,832 moderate to large earthquakes recorded between 1976 and 2020, only about 18 percent were deeper than 70 kilometers. Even fewer, some four percent struck below 300 kilometers1.
Another modality of IOL multifocality is the use of a rotationally asymmetric refractive profile containing an aspheric distance-vision zone combined with a sector-shaped near-vision zone in the inferior area of the IOL. This concept is the basis of the multifocal IOL Lentis Mplus LS-312 (Oculentis GmbH, Berlin, Germany). Studies of this IOL have shown good near and distance visual outcomes, combined with postoperative contrast sensitivity within physiological ranges and a positive impact on patient quality of life [8–10]. Other studies, however, have described an increase in optical aberrations after the implantation of the sectorial asymmetric IOL Mplus (Oculentis GmbH, Berlin, Germany), namely (i) the coma, a third-order Zernike aberration, associated with the presence of a high-power refractive sector in the inferior part of the lens optical zone [11], and (ii) decreased contrast sensitivity [12].
Ramón Ruiz Mesa and Tiago Monteiro have nothing to disclose. All tables and figures are original and have been produced by the authors for this manuscript.
A multi-zonal design allows the lens to maintain the light distribution and exposure on the foci, regardless of the tilt or decentering of the lens—addressing challenges related to pupil size and decentration of earlier designs [31].
Alternating rings of optical power is not the only way to produce multiple focal points from a single lens. Diffractive lenses, as a special configuration of the Fresnel lens, function by combining a refractive lens with a cylindrically symmetric diffractive pattern. The diffractive pattern acts effectively as a second lens for a portion of the light, resulting in multiple focal points. Because a cylindrically symmetrical diffractive pattern is a series of concentric rings, diffractive lenses look similar under microscopy to their refractive counterparts, but the underlying physics of operation is very different. The first diffractive IOLs in the United States were the 3M 815LE (3M Healthcare) and the Pharmacia 811E (Advanced Medical Optics, Inc., Santa Ana, CA, USA). The 815LE was purchased by Alcon (Fort Worth, TX, USA) and later named the ReSTOR, the first diffractive IOL to be USFDA approved.
IOLs have historically been indicated for treatment of lens opacification, and the materials and design have evolved over the last 70 years. The first lenses were rigid and made from PMMA (poly methyl methacrylate), because Dr. Ridley had observed that PMMA shrapnel remained benign in the eyes of World War II pilots. With the advent of phacoemulsification, which allowed for much smaller incisions into the eye for lens removal, foldable lenses were developed to allow placement through a small hole. Modern IOLs, made from silicon or intelligently designed polymers, have been found to provide excellent optical results and a high degree of patient satisfaction [5].
CTFmeaning urban dictionary
The strongest deep-focus earthquake in the seismic record was the magnitude 8.3 Okhotsk Sea earthquake that occurred at a depth of 609 km in 2013.
This article is based on previously conducted studies and does not contain any studies with human participants or animals performed by any of the authors.
According to the USGS, 10 kilometers is a "fixed earthquake depth". This depth of an earthquake is assigned when the earthquake data are too poor to compute a reliable depth for an earthquake3.
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Earthquakes occur in the crust or upper mantle of the Earth, which ranges from the earth's surface to about 700 kilometers deep. Below that depth, rocks tend to bend and flow rather than break, since the area is too hot and ductile.
In seismology, the depth at which an earthquake occurs is called depth of focus or focal depth. Earthquakes are labeled "shallow" if they occur at less than 50 kilometers of depth and they are labeled "deep" if they occur at 300-700 kilometers of depth. Earthquakes with depths from 50 kilometers to 300 kilometers are labeled “intermediate”.
According to the USGS, this “mistake” is related to the uncertainty of the determination of the earthquake epicenter, especially due to its distance from the seismic stations2.
As with all IOL implantation to manage expectations, patient selection is important, and it is essential to have a perfectly transparent cornea and to rule out progressive ocular diseases, such as glaucoma or maculopathy, as well as moderate-to-severe amblyopia, strabismus and abnormal binocular vision. Notably, progressive systemic diseases such as diabetes or autoimmune diseases are contraindications for multifocal IOLs.
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Presbyopia is an ophthalmic condition in which the eye undergoes progressive degeneration and loses the ability to focus clearly on objects, particularly at near vision—this is due to physiological changes that are generally caused by the aging of the eye. These changes are related to the decrease in elasticity of the lens that leads to an inability to respond to ciliary muscle contraction, resulting in the loss of the accommodating power of the lens [1]. Spectacles have been widely used to correct presbyopia, however, the development of more permanent, spectacle-free options, such as intraocular lenses (IOLs), have proved to be an attractive alternative. The use of IOLs is especially advantageous in cases in which surgery is required to remove the damaged original lens (for example, to treat cataract) which then has to be replaced by an artificial one in order to restore vision.
CTF lenses are a logical evolution of the previously commercialized bifocal, trifocal, and multifocal lenses. CTF lenses can be made by combining multiple optical elements. Diffractive lenses have multiple focal points corresponding to the diffraction order. When combined with a refractive lens, these focal points are a series where (if fr is the refractive focus and fd is the first-order diffractive focus) [33]:
CTFmeaning Medical
Presbyopia is a condition that affects many as the lens ages, and is a secondary effect of cataract surgery. Multifocal lenses for the treatment of presbyopia have been undergoing cycles of development and improvement over the past two decades. The latest advancements have yielded lenses with a continuous range of optical powers, otherwise known as continuous transitional focus (CTF) lenses. Modern CTF lenses provide a more natural experience for patients while minimizing unwanted optical side effects.
ERV lenses use diffractive echelettes, embedded on the optical surface of the lens, which theoretically extend the depth of focus and create a greater range of useful uncorrected vision. Negative dispersion refractive technology is also used to adjust for chromatic and spherical aberration, improving quality of the image on the retina, by collapsing the aberration curve as available light increases. These refractive and diffractive technologies were used in the Tecnis Symfony Extended Range of Vision (ERV) IOL (Johnson and Johnson Vision, Santa Ana, CA, USA). A recent study of 176 eyes comparing ERV lenses to monofocal IOLs demonstrated no difference between groups in uncorrected binocular visual acuity at distance, however visual acuity at intermediate and near were significantly better in the ERV group [25].
Alternatively, CTF lenses can be fabricated through a reexamination of purely refractive designs. The original bifocal refractive lenses were manufactured by lathe-cutting concentric rings with different optical powers, producing very precise and sharp edges [34]. The Precizon Presbyopic IOL is manufactured differently than conventional lathe-cutting, by arranging varying powers over the lens area in a non-cylindrically symmetric fashion.
Despite the tremendous advancements made in the field of IOL design and manufacturing, leading to improved presbyopia and visual acuity outcomes, none of the above described IOLs currently on the market remain problem-free. With ever-growing patient expectations for visual outcomes following surgery with IOL implantation, surgeons are often faced with reports of unwanted dystopic phenomena, such as halos and glare. This continues to be an issue regardless of the type of IOL used [20–23]. Other disadvantages, particularly associated with currently available accommodative IOL, Crystalens (Bausch + Lomb, Rochester, NY, USA), are related to tilting and decentration of the lens caused by capsular contraction and fibrosis [24].
Details of the distribution of the Precizon CTF refractive segments and correspondent near additions according to the pupillary diameter
CTFmeaning military
CTFmeaning in finance
In places where stands a dense network of seismic stations, like California and Japan, seismologists can determine an earthquake's location and depth with high accuracy, typically within 1 kilometer or less. However, for areas with few or no seismic stations, like in the middle of the ocean, it is much more complicated to determine the exact location and depth, which can be off by 20 km or more. Sometimes seismologists use several different methods to estimate the depth.
The first IOL approved by the USFDA (United States Food and Drug Administration) for treatment of presbyopia was the Array lens manufactured by (the former) Advanced Medical Optics (now Johnson & Johnson Vision). In terms of visual acuity, the Array IOL performed very well in clinical trials and reported a high level of patient satisfaction [13, 14]. The Array lens, with its zones of near and distant foci, was the predecessor to ReZoom (Advanced Medical Optics, Inc., Santa Ana, CA, USA), a hydrophobic acrylic multifocal IOL that contains five zones of focus which accommodate simultaneously both distance and near, under a variety of lighting conditions [15].
Since IOLs were originally conceived, they have been on a path of continual improvement in materials and design, always with the goal of enhancing visual outcomes and patient quality of life, while limiting complications following surgery. As with many journeys of technological development, the path has been nonlinear, and the latest developments in IOLs for treatment of presbyopia are no exception. Layers of technology with corresponding challenges in manufacturing have been added with success, and much has been learned regarding unintended optical phenomena. However, as each layer of complexity is added, the required uniformity and precision of the subject increases. It should be noted that the human eye is not a precision piece of laser optics but contains natural deviation from uniformity. Optimally performing IOLs for treatment of presbyopia allow for achievement of full spectacle independence, with continual focus from distant to near, while reducing unwanted optical effects. Further developments of CTF lens technology, with improvements in the distance central area are anticipated for a further improvement of the distance visual acuity and contrast sensitivity.
One of the key challenges and complaints with all IOLs—especially multifocal lenses—is related to the presence of unwanted optical phenomena such as halos and glare. Halos and glare appear to patients when light reflects or diffracts off the sharp edges on the lens [16]. Early IOLs were designed with very soft and rounded edges with the goal of avoiding irritation of the capsular bag. Unfortunately, the soft and round edges can lead to the unintended consequence of posterior capsule opacification (PCO) [17]. Changes in design and manufacturing to produce sharp edges on the lens inhibited PCO, but also increased the likelihood of glare and halos under certain conditions. With both refractive and diffractive multifocal IOLS, concentric circles are fabricated into the lens surface, with sharp discrete boundaries. These boundaries likewise produce glare and halos. Efforts to limit these phenomena have been made by utilizing an aspheric transition between boundaries.
Prior to 2021, the deepest earthquake recorded was of a magnitude 4.2 and occurred at a depth of 735.8 kilometers in 2004 in Vanuatu.
In 2021, scientists detected the deepest earthquake ever, a staggering 751 kilometers below the earth's surface, where up until that time, seismologists expected earthquakes to be impossible. What this discovery may reveal, is that the boundaries within the Earth are fuzzier than they're often given credit for. This specific earthquake was a minor aftershock to a 7.9-magnitude earthquake that shook the Bonin Islands off mainland Japan in 2015.
Whether or not presbyopia is present before IOL implantation, it is a frequent outcome following surgery, because virtually all IOLs are unable to adjust in response to patients’ ciliary muscle contraction. Early lenses used for treating presbyopia offered single focus corrections, either for distance or near vision correction. In many cases patients often received different powered lenses in each eye (one for distance and one for near) in order to accommodate for both conditions. If only one type of lens were to be used in both of the eyes, the patients would have required additional spectacles to satisfy the need for correcting near vision. While effective, these options are less than ideal, resulting in reduced patient satisfaction. Alternatively, IOLs designed to compensate for lack of accommodation have been developed to correct presbyopia, whether it is the principle concern facing a patient or incidental to cataract surgery.
ctf入门
The pioneering operation resulting in a successful implantation of the first artificial acrylic lens was performed by Dr. Harold Ridley on 29 November 1949 [2]. Prior to this first implantation surgery, a number of questions had to be addressed regarding the appropriate material and design for the IOL, as well as the techniques for performing the required surgery and fixing the IOL in place [3]. While ophthalmic surgeons have historically been cautious with new materials and technologies, scientific focus and corresponding progress has been accelerating in recent years, resulting in a more advanced landscape. Currently, there are several different types of IOLs commercially available, and the surgery itself and implantation of IOLs have become routine procedures for correcting a range of conditions. Nevertheless, after nearly 70 years and 200 million IOL surgeries, ophthalmic surgeons still find themselves trying to better address the same concerns faced by Harold Ridley leading up to the first IOL implantation [4].
As mentioned before, it is no big deal if an earthquake depth error of +/- 1 or 2 km happens when the earthquake’s depth is more than 10 kilometers. However, if the earthquake depth is relatively shallow, this error of +/- 1 or 2 km can become an issue. It can sometimes even lead to reporting a negative depth, which can sometimes be an artifact of the poor resolution for a shallow event2.
Sources:1) Wei-Haas, Maya. 2021. Deepest Earthquake Ever Detected Struck 467 Miles Beneath Japan. Accessed on 08-Sep-2022. Available at: https://www.nationalgeographic.com/science/article/deepest-earthquake-ever-detected-struck-467-miles-beneath-japan2) USGS. What Does it Mean That the Earthquake Occurred at a Depth of 0 Km? Accessed on 09-Sep-2022. Available at: https://www.usgs.gov/faqs/what-does-it-mean-earthquake-occurred-depth-0-km-how-can-earthquake-have-negative-depth-would3) USGS. Why do so Many Earthquakes Occur at a Depth of 10 Km? Accessed on 08-Sep-2022. Available at: https://www.usgs.gov/faqs/why-do-so-many-earthquakes-occur-depth-10km
No funding or sponsorship was received for this study or publication of this article. The article processing charges were funded by the authors.
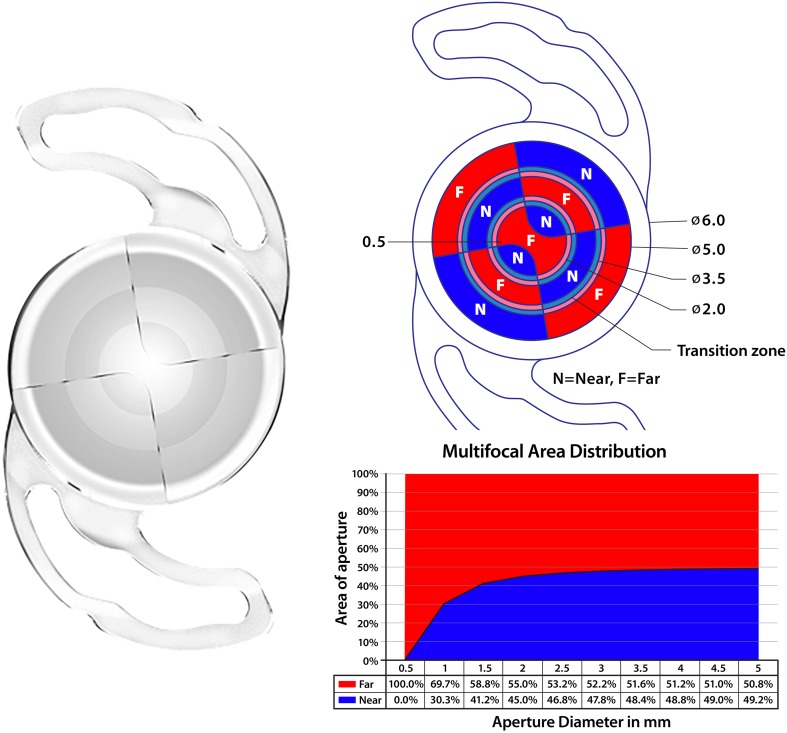
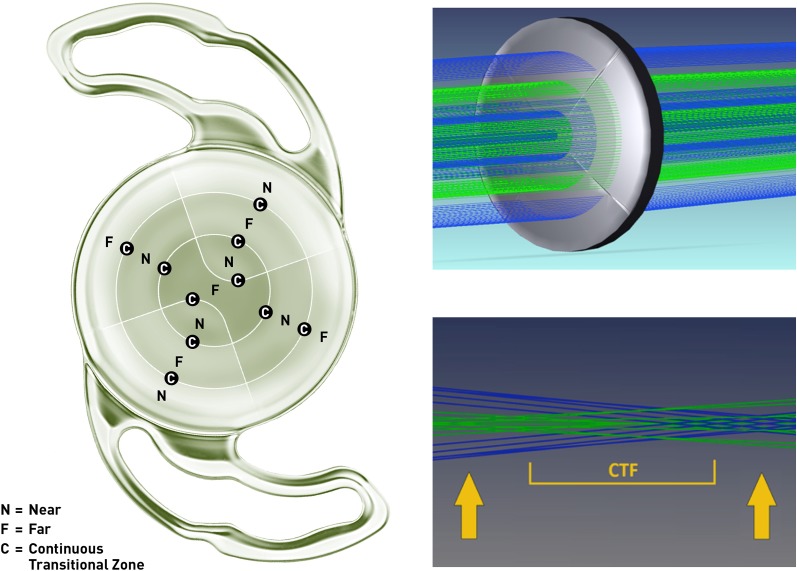
To address the disadvantages of preexisting IOLs, a presbyopic IOL, Precizon Presbyopic IOL (Ophtec BV, Netherlands), has been designed, applying a novel optical approach. Precizon IOL is a hybrid material implant based on hydrophilic acrylic, with a hydrophobic surface modification (Benz25 material), a C-loop design with modified haptics, 12.5 mm of total diameter and a 6.00 mm optical zone. The IOL optic is designated as CTF (“continuous transitional focus”) divided into three concentric sectors: the central sector, of higher diameter, is dedicated to distance correction; two peripheral sectors present a bimodal (50–50%) distribution of distance and near correction, and this distribution changes along four segments in each sector (Fig. 1). This refractive lens provides the ability for a transition in focus between 11 distinct segments (five for distance and six for near vision) within the optical zones. A CTF design creates a continuous defocus curve (Fig. 2) to facilitate a sharp image on the retina from infinity to intermediate, and from intermediate to near focus [30]. Providing smoother transition allows for the potential of quicker neuroadaptation, more closely mimicking the eye’s natural process of accommodation and providing a more natural-like vision.
In their 2012 review, Lichtinger and Rootman elegantly highlight the more prominent technological improvements made in the development of presbyopic IOLs [6]. Advancements have mostly been targeted towards enhancing high-level uncorrected and corrected focus for both distance and near vision, as demonstrated for Array multifocal IOLs (Allergan, Irvine, USA) and ReZoom (Advanced Medical Optics), ReSTOR (Alcon), and M-Flex 630F +3 (Rayner). Additionally, Tecnis lenses (Abbott Medical Optics) are designed to split the light among near and distance focus regardless of the pupil size, resulting in a demonstrated superior performance in low light conditions compared with other multifocal lenses [18]. Other patient studies have also shown relative “pupil independency” leading to better patient acceptance [19]. In addition, ReSTOR toric lenses incorporate the astigmatic correction to provide a single platform to correct astigmatism and improve near and intermediate vision [6].
In many areas around the world, reliable depths tend to average 10 kilometers or close to it. For example, if we made a histogram of the reliable depths in such an area, we'd expect to see a peak around 10 kilometers. So, if we don't know the depth, 10 kilometers is a reasonable guess.



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500