
IEC metric screw sized connectors - m12 cable pinout
Zhao Y, Xiong J, Hou Y, Zhu M, Lu Y, Xu Y, et al. Early detection of ST-segment elevated myocardial infarction by artificial intelligence with 12-lead electrocardiogram. Int J Cardiol 2020;317:223–230.
The rear aperture or exit pupil of the objective restricts the light rays as they pass through an objective. The diameter of this aperture varies between 12 millimeters for low magnification objectives down to around 5 millimeters for the highest power apochromatic objectives. Close consideration of aperture size is absolutely imperative for epi-illumination applications that rely on the objective to act as both an imaging system and condenser, where the exit pupil also becomes an entrance pupil. The image of the light source must entirely fill the objective rear aperture to produce even illumination across the viewfield. If the light source image is smaller than the aperture, the viewfield will experience vignetting from uneven illumination. Conversely, if the light source image is larger than the rear aperture, all of the light will not enter the objective and the intensity of illumination is reduced.
1.1.02-129
The distance from the lens center to a point where parallel rays are focused on the optical axis is defined as the focal length of a lens system. An imaginary plane perpendicular to the principal focal point is called the focal plane of the lens system. There are two principal focal points, one in front and one at the rear, for light entering each side of every lens. Conventionally, the objective focal plane found nearer to the front lens element is known as the front focal plane and the focal plane located behind the objective is known as the rear focal plane. The specific position of the rear focal plane varies with construction of the objective, but is usually situated somewhere inside the objective barrel for high magnification objectives. Lower magnification objectives often have a rear focal plane that is located on the exterior, in the thread area or within the microscope nosepiece.
Ha SH, Joo SH. A hybrid data mining method for the medical classification of chest pain. Int J Comput Inf Eng 2010;4:99–104.
Green M, Björk J, Forberg J, Ekelund U, Edenbrandt L, Ohlsson M. Comparison between neural networks and multiple logistic regression to predict acute coronary syndrome in the emergency room. Artif Intell Med 2006;38:305–318.
Harrison RF, Kennedy RL. Artificial neural network models for prediction of acute coronary syndromes using clinical data from the time of presentation. Ann Emerg Med 2005;46:431–439.
In many biological and petrographic applications, when mounting the specimen, a glass coverslip is used to both protect the integrity of the specimen and to provide a clear window for observation. The coverslip acts to converge the light cones originating from each point in the specimen. But it also introduces chromatic and spherical aberration that must be corrected by the objective. The refractive index, dispersion, and thickness of the coverslip determine the degree to which light rays are converged. An additional concern is the aqueous solvent or excess mounting medium that lies between the specimen and coverslip in wet or thickly mounted preparations, which add to the variations in refractive index and thickness of the cover slip.
It is possible to correct for variations in coverslip thickness. Several high-performance apochromat dry objectives are fitted with correction collars that allow adjustment by a rotating collar, which causes two of the lens element groups in the objective to move closer together or farther apart (see Figure 4). Various specialized phase contrast objectives that are designed for tissue culture observation with an inverted microscope have an even broader compensation range of between 0 to 2 millimeters. In this way, specimens can be viewed through the bottom of most culture vessels, which in this size range, often have dramatic thickness fluctuations.
Performance of the occlusion myocardial infarction artificial intelligence model and analysis of different occlusion myocardial infarction outcome definitions across the grouped testing data sets (both Europe and USA)
A majority of acute coronary syndromes (ACS) present without typical ST elevation. One-third of non–ST-elevation myocardial infarction (NSTEMI) patients have an acutely occluded culprit coronary artery [occlusion myocardial infarction (OMI)], leading to poor outcomes due to delayed identification and invasive management. In this study, we sought to develop a versatile artificial intelligence (AI) model detecting acute OMI on single-standard 12-lead electrocardiograms (ECGs) and compare its performance with existing state-of-the-art diagnostic criteria.
202326 — The documentation on the Catalyst 9800 CL says maximum APs per site is 100. Is this correct? Does this mean i can only have 100 Ap's in a single office this ...
Wu L, Huang G, Yu X, Ye M, Liu L, Ling Y, et al. Deep learning networks accurately detect ST-segment elevation myocardial infarction and culprit vessel. Front Cardiovasc Med 2022;9:797207.
A total of 18 616 ECGs from 10 543 patients (age 66 ± 14 years, 65.9% males, 22.9% OMI) with clinically validated outcomes originating from the Cardiovascular Centre Aalst and an international image database of ACS patients were included in the AI model development. The sample characteristics are shown in Table 1.
Microscope manufacturers produce objectives with restricted tolerances to refractive index and dispersion. This means they require matching values in the liquid placed between the coverslip and objective front lens. It is advisable to employ only the oil intended by the objective manufacturer, and to not mix immersion oils between manufacturers. Additionally, objectives that use water and/or glycerin as an imaging medium are also available for applications with living cells in culture or sections of tissue immersed in physiological saline solution.
Values in bold indicate statistically significant differences (p < 0.05). Cat., category; CAG, coronary angiography; ECG, electrocardiogram; STEMI, ST-elevation myocardial infarction; SD, standard deviation; LMCA, left main coronary artery; LAD, left anterior descending artery; LCx, left circumflex artery; NA, not available; RCA, right coronary artery; PDA, posterior descending artery; RI, ramus interventricularis; TIMI, Thrombolysis in myocardial infarction; PCI, percutaneous coronary intervention.
where Resolution is the minimum separation distance between two point objects that are clearly resolved, λ is the illumination wavelength, n is the imaging medium refractive index, and θ is equal to one-half of the objective angular aperture. With this in mind, it is apparent that resolution is directly proportional to the illumination wavelength. The human eye responds to the wavelength region between 400 and 700 nanometers, which represents the visible light spectrum that is utilized for a majority of microscope observations. Resolution is also dependent upon the refractive index of the imaging medium and the objective angular aperture. Objectives are intended to image specimens either through air or a medium of higher refractive index between the front lens and the specimen. The field of view is often highly restricted, and the front lens element of the objective is placed close to the specimen with which it must lie in optical contact. A gain in resolution by a factor of about 1.5 is attained when immersion oil is substituted for air as the imaging medium.
Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction. J Am Coll Cardiol 2018;72:2231–2264.
Finally, the last but perhaps most important factor in determining the resolution of an objective is the angular aperture, which has a practical upper limit of about 72 degrees (with a sine value of 0.95). When combined with refractive index, the product:
The primary outcome was the AI model’s ability to identify patients with angiographically confirmed OMI using only single-standard 12-lead ECGs. The primary definition of OMI was modelled from previous studies2,5,9,10,17–19 and consisted of clinical symptoms and a troponin elevation consistent with the fourth universal definition of MI20 and angiographic evidence of acute culprit coronary stenosis with either (i) a thrombolysis in myocardial infarction (TIMI) flow grade of 0–1 or (ii) a TIMI flow grade of 2–3 with emergent or urgent percutaneous revascularization. Patients without any dynamic changes detected in serial biomarker testing were safely ruled out for OMI regardless of undergoing coronary angiography. This outcome was considered the reference standard for all analyses unless otherwise specified.
Dodd KW, Zvosec DL, Hart MA, Glass G III, Bannister LE, Body RM, et al. Electrocardiographic diagnosis of acute coronary occlusion myocardial infarction in ventricular paced rhythm using the modified Sgarbossa criteria. Ann Emerg Med 2021;78:517–529.
A real-world demonstration of an occlusion myocardial infarction artificial intelligence true-positive electrocardiogram downloaded from Twitter. (A) The original electrocardiogram posted to Twitter by Brooks Walsh, MD (https://twitter.com/BrooksWalsh, emergency physician at the Bridgeport Hospital, Bridgeport, CT, USA) with the occlusion myocardial infarction artificial intelligence model interpretation (above the optimal threshold); (B) the occlusion myocardial infarction artificial intelligence electrocardiogram model interpretation (above optimal threshold) with model explainability; (C) the angiogram of the occluded proximal left circumflex culprit artery and high-sensitivity troponin T evolution for this case.
In situations where the specimen is designed to be imaged without a coverslip, the working distance is measured at the actual surface of the specimen. Working distance typically decreases in a series of matched objectives as the magnification and numerical aperture increase. Objectives intended to view specimens with air as the imaging medium should have comparatively long working distances providing that numerical aperture requirements are satisfied. Alternatively, immersion objectives should have shallower working distances in order to keep the immersion liquid between the front lens and the specimen in place. Many objectives designed with similar working distances have a spring-loaded retraction stopper that allows the front lens assembly to be withdrawn by pushing it into the objective body and twisting to secure its place. Twisting the retraction stopper in the opposite direction releases the lens assembly for use. In some applications (see below), a long free working distance is indispensable, and special objectives are designed for such use despite how difficult it is to achieve large numerical apertures and the necessary degree of optical correction.
Worauf müssen Sie sich hier einstellen
OMI, occlusion myocardial infarction; AI, artificial intelligence; STEMI, ST-elevation myocardial infarction; Sens., sensitivity; Spec., specificity; PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; MCC, Matthew’s correlation coefficient; TIMI, thrombolysis in myocardial infarction; Trop, troponin; PCI, percutaneous coronary intervention.
Pride YB, Tung P, Mohanavelu S, Zorkun C, Wiviott SD, Antman EM, et al. Angiographic and clinical outcomes among patients with acute coronary syndromes presenting with isolated anterior ST-segment depression: a TRITON–TIMI 38 (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition With Prasugrel–Thrombolysis In Myocardial Infarction 38) substudy. JACC Cardiovasc Interv 2010;3:806–811.
The OMI AI model was compared against two standard criteria assessing the same 12-lead ECGs in the overall test set for the presence of OMI (Table 4). At the optimal threshold, the OMI AI model exhibited a significantly higher sensitivity in identifying OMI compared with STEMI criteria [80.6% (95% CI: 76.8–84.0%) vs. 32.5% (95% CI: 28.4–36.6%), P < 0.001] and was statistically equal to ECG experts [73.0% (95% CI: 68.7–77.0%)]. Accuracy in detecting OMI was equal between the OMI AI model and the experts and significantly higher when compared with STEMI criteria. Specificity was highest for STEMI criteria [97.7% (95% CI: 97.0–98.3%)] compared with ECG experts [95.7% (95% CI: 94.7–96.6%)] and OMI AI model [93.7% (95% CI: 92.6–94.8%)]. The comparison of all independently tested criteria for OMI diagnosis is summarized in Supplementary material online, Table S1.
Warum müssen Sie vor dem Rechtsabbiegen warten
For several years, most manufacturers conformed to an international standard of parfocal distance when designing objective lenses for biological applications. As a result, a majority of objectives had a parfocal distance of 45.0 millimeters and were considered interchangeable. As it became commonplace to produce infinity-corrected tube lengths, a new set of design criteria was created to correct for aberrations in the objective and tube lenses. Alongside a demand for greater flexibility to accommodate the requirement of expanding working distances with higher numerical apertures and field sizes, interchangeability between objective lenses from different manufacturers is now more limited.
VEICHI at SPS Italia 2024, Fiere di Parma Fairgrounds, Parma, Italy on 28-30 May, 2024.
Wu C-C, Hsu W-D, Islam MM, Poly TN, Yang H-C, Nguyen P-AA, et al. An artificial intelligence approach to early predict non-ST-elevation myocardial infarction patients with chest pain. Comput Methods Programs Biomed 2019;173:109–117.
Conflict of interest: R.H. is the co-founder and Chief Medical Officer of Powerful Medical; M.M., J.B., A.I., B.V., V.B., V.K., and A.D. are employees and shareholders of Powerful Medical. S.W.S., H.P.M., and L.P. are shareholders in Powerful Medical.
Worauf müssen Sie innerorts an Kreuzungen und Einmündungen besonders achten
These beam splitters are used when the polarization of the light changes or when the same reflection is required for both polarization states.
Forberg JL, Green M, Björk J, Ohlsson M, Edenbrandt L, Öhlin H, et al. In search of the best method to predict acute coronary syndrome using only the electrocardiogram from the emergency department. J Electrocardiol 2009;42:58–63.
Recently, a machine learning approach has outperformed standard ECG criteria in detecting acute OMI correlating 73 hand-selected morphological ECG features and clinical parameters.16 In this study, we introduce an international validation of an automated deep learning artificial intelligence (AI) model detecting acute OMI using only a single-standard 12-lead ECG as input and hypothesize that it would outperform the existing state-of-the-art ECG criteria for the detection of acute OMI and match the performance of interpreters with special expertise in ECG OMI diagnosis.
The common design of a practical oil immersion objective includes a hemispherical front lens element, followed by a positive meniscus lens and a doublet lens group. Aplanatic refractions occur at the first two lens elements in a typical apochromatic oil immersion objective. Oil immersion objective lenses can also correct for chromatic defects that are introduced by the first two lens elements, while initiating a minimum amount of spherical aberration. Employing an oil immersion objective without oil between the cover slip and first lens element will result in defective images due to refraction that cannot be corrected by subsequent lens components within the objective.
The key difference is that unpolarized light has vibrations in multiple planes, whereas polarized light has vibrations in only one plane.
Wang TY, McCoy LA, Bhatt DL, Rao SV, Roe MT, Resnic FS, et al. Multivessel vs culprit-only percutaneous coronary intervention among patients 65 years or older with acute myocardial infarction. Am Heart J 2016;172:9–18.
Wagner GS, Macfarlane P, Wellens H, Josephson M, Gorgels A, Mirvis DM, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part VI: acute ischemia/infarction a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol 2009;53:1003–1011.
Ref, reference; OMI, occlusion myocardial infarction; AI, artificial intelligence; STEMI, ST-elevation myocardial infarction; PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; ECG, electrocardiogram.
2024715 — Vision inspection systems play a crucial role in ensuring quality assurance and compliance within manufacturing processes. By employing advanced ...
Oxford University Press is a department of the University of Oxford. It furthers the University's objective of excellence in research, scholarship, and education by publishing worldwide
Several limitations are to be considered. Although validated in multi-centre, international cohorts of patients, our study lacks prospective validation. In clinical practice, the decision to refer for early angiography in patients presenting with NSTEMI, as well as to treat by revascularization or conservatively, is based not only on ECG but often encompasses additional clinical criteria. Nevertheless, our results show less than half (43.9%) of OMI patients undetected by standard STEMI criteria that could have had accelerated access to PCI based on the AI model detection truly underwent revascularization within 2 h. However, their median time to revascularization was delayed by over 9 h. There were significant differences in clinical presentation and management between patients in the Europe and USA due to variations in the standard of care. Although the model has demonstrated robust performance across various subgroups, its sensitivity was lower in patients with left bundle branch block and broad QRS morphology. The outcome of OMI relied on a visual verification of TIMI flow on angiograms, which may be subjective when compared with TIMI frame counting, and was not performed in an independent core lab. Culprit lesions with TIMI 2/3 flow requiring urgent revascularization were encompassed in the primary outcome since up to one-fourth of STEMI patients have pharmacological or spontaneous reperfusion at the time of angiography. In this regard, we present an AI model performance, utilizing broad ranges of peak troponin cut-offs, which may serve as more appropriate indicators of significant myocardial infarction resulting from these lesions. The OMI AI model detects OMI with a binary granularity. It is understood that the different stages of culprit coronary lesion leading to ACS, in terms of dynamics (active or reperfused) and time (acute or subacute), can have an influence on patient outcomes and the timing of invasive strategies. Lastly, our study is not generalizable to a broader population of asymptomatic patients and was not designed to quantify other relevant clinical endpoints such as mortality, in-hospital complications, or major adverse cardiovascular events (MACE). Future work should address these limitations and observe the AI model efficacy and clinical benefit deployed in a prospective cohort of ACS patients.
When the objective is assembled, spherical aberration is corrected by selecting the best set of spacers to fit between the hemispherical and meniscus lens (the lower lens mounts). The objective is parfocalized by translating the entire lens cluster upward or downward within the sleeve with locking nuts so that focus will not be lost while objectives housed on a multiple nosepiece are interchanged. Adjustment for coma is accomplished with three centering screws that optimize the position of internal lens groups with respect to the optical axis of the objective.
Patients with an acutely occluded or obstructive culprit coronary artery (acute coronary occlusion myocardial infarction, abbreviated as ‘OMI’), who will benefit from emergent reperfusion therapy, are currently identified on the basis of electrocardiographic ST-segment elevation [ST-elevation myocardial infarction (STEMI)].1,2 However, the pathophysiology of acute coronary syndrome (ACS) due to thrombotic occlusive coronary stenosis is often dynamic and may impact electrocardiogram (ECG) appearance at the time of the first patient contact. Accordingly, growing evidence suggests that the current ACS classification dichotomizing patients as STEMI or non-STEMI (NSTEMI) is unsatisfactory for the timely diagnosis of OMI, as also recognized by the 2022 American College of Cardiology Chest Pain Expert Consensus.3 On the one hand, 25–30% of NSTEMI patients present with acute coronary occlusion with insufficient collateral circulation as discovered only on delayed coronary angiography (CAG).4 The delayed invasive management in these patients is associated with two-fold higher short-term and long-term mortality.4,5 On the other hand, 15–25% of catheterization laboratory activations due to suspected STEMI eventually reveal no culprit lesions or a non-ischaemic aetiology of ST elevation (STE).6–8 A plethora of ECG criteria have been proposed to increase diagnostic sensitivity for OMI compared with the current guideline–based STEMI criteria and to differentiate OMI from mimics.3,5,9–15 Yet, their adoption is limited due to their complexity and unclear inter-evaluator reliability.
Takeda M, Oami T, Hayashi Y, Shimada T, Hattori N, Tateishi K, et al. Prehospital diagnostic algorithm for acute coronary syndrome using machine learning: a prospective observational study. Sci Rep 2022;12:14593.
Values in bold indicate statistically significant differences (p < 0.05). Cat., category; CAG, coronary angiography; ECG, electrocardiogram; STEMI, ST-elevation myocardial infarction; SD, standard deviation; LMCA, left main coronary artery; LAD, left anterior descending artery; LCx, left circumflex artery; NA, not available; RCA, right coronary artery; PDA, posterior descending artery; RI, ramus interventricularis; TIMI, Thrombolysis in myocardial infarction; PCI, percutaneous coronary intervention.
Artificial intelligence model performance on the overall testing data set. The receiver operating characteristic curve of the occlusion myocardial infarction artificial intelligence model (red) and the sensitivity and specificity of the occlusion myocardial infarction artificial intelligence model optimal threshold (red X), STEMI criteria (green dot), and electrocardiogram experts (purple cross) on combined EU and US testing cohorts. The AUC is 0.938 [n = 2263 contacts (21.61% occlusion myocardial infarction)]. OMI, occlusion myocardial infarction; AI, artificial intelligence; STEMI, ST-elevation myocardial infarction.
For many years, field curvature went uncorrected as the most severe optical aberration that occurred in fluorite (semi-apochromat) and apochromat objectives, tolerated as an unavoidable artifact. The introduction of flat-field (plan) correction to objectives perfected their use for photomicrography and video microscopy, and today these corrections are standard in both general use and high-performance objectives. Figure 3 illustrates how correction for field curvature (for a simple achromat) adds a considerable number of lens elements to the objective. The significant increase in lens elements for plan correction also occurs with fluorite and apochromat objectives, frequently resulting in an extremely tight fit of lens elements (see Figure 1) within the internal objective sleeve.
Electrocardiogram and outcome data from the Diagnosis of Occlusion MI And Reperfusion by Interpretation of the electrocardioGram in Acute Thrombotic Occlusion (DOMI ARIGATO) database (clinical trials.gov number NCT03863327) were included in the US external testing cohort. Data collection and processing of this database are explained elsewhere.2 Briefly, the DOMI ARIGATO database collected ECGs, laboratory data, and the clinically verified angiograms of patients presenting with ACS at two US sites, Stony Brook University Hospital and Hennepin County Medical Center. Electrocardiograms were interpreted and manually annotated by ECG experts blinded to all clinical data other than age and sex. Baseline ECGs, post-CAG ECGs, and ECGs with missing expert annotations were removed from the testing cohort.
Al-Zaiti SS, Martin-Gill C, Zègre-Hemsey JK, Bouzid Z, Faramand Z, Alrawashdeh MO, et al. Machine learning for ECG diagnosis and risk stratification of occlusion myocardial infarction. Nat Med 2023;29:1804–1813.
Figueras J, Otaegui I, Marti G, Domingo E, Bañeras J, Barrabés JA, et al. Area at risk and collateral circulation in a first acute myocardial infarction with occluded culprit artery. STEMI vs non-STEMI patients. Int J Cardiol 2018;259:14–19.
The most important imaging component in the optical microscope is the objective, a complex multi-lens assembly that focuses light waves originating from the specimen and forms an intermediate image that is subsequently magnified by the eyepieces. Objectives are responsible for primary image formation and play a central role in establishing the quality of images that the microscope is capable of producing. Furthermore, the magnification of a particular specimen and the resolution under which fine specimen detail also heavily depends on microscope objectives. The most difficult component of an optical microscope to design and assemble, the objective is the first element that light encounters as it passes from the specimen to the image plane. Objectives received name from the fact that they are, by proximity, the closest component to the object, or specimen, being imaged.
In the past 100 years, construction techniques and materials used to manufacture objectives have greatly improved. Composed up of numerous internal glass lens elements, modern objectives have reached a high state of quality and performance considering the extent of correction for aberrations and flatness of field. Objectives are currently designed with the assistance of Computer-Aided-Design (CAD) systems, which use advanced rare-element glass formulations of uniform composition and quality characterized by highly specific refractive indices. These advanced techniques have allowed manufacturers to produce objectives that are very low in dispersion and corrected for most of the common optical artifacts such as coma, astigmatism, geometrical distortion, field curvature, spherical and chromatic aberration. Not only are microscope objectives now corrected for more aberrations over wider fields, but image flare has been dramatically reduced thanks to modern coating technologies, with a substantial increase in light transmission, yielding images that are remarkably bright, sharp, and crisp.
Al-Zaiti S, Besomi L, Bouzid Z, Faramand Z, Frisch S, Martin-Gill C, et al. Machine learning-based prediction of acute coronary syndrome using only the pre-hospital 12-lead electrocardiogram. Nat Commun 2020;11:1–10.
Clinical data from 9764 patients who presented with suspected ACS to the Cardiovascular Centre Aalst in Belgium during the period between 2011 and 2021 and a clinically validated international image database of 2368 ACS patients (see Supplementary material online for a detailed description) were considered for the AI model development and testing. Waveform data, sampled at 500 Hz, were exported from the MUSE ECG data management system (GE Healthcare, Chicago, IL, USA) in XML format. The images of ECG tracings from multiple device vendors within the international image database of ACS patients were converted to digital waveforms using Ce-certified PMcardio ECG digitization technology (Powerful Medical, Samorin, Slovakia). Electrocardiograms recorded >24 h before CAG and post-CAG or ECGs with poor signal quality were discarded. The patients retained upon exclusions were randomly split into a model development (derivation) set and an internal Europe (EU) testing data set, ensuring that patients with more than one (recurrent) ACS contact were present in only one of the sets. Time from the first ECG to intervention was recorded for all cases if the patients underwent coronary angiography. The derivation set included ECGs adjudicated as OMI or not OMI by interpreters with special expertise in ECG OMI diagnosis (S.W.S. and H.P.M.) and by clinically validated angiographic outcome data (see details below under ‘Occlusion myocardial infarction artificial intelligence model development’). ‘Not OMI’ encompasses patients who either do not have acute myocardial infarction (MI) or have acute non-occlusion MI (non-OMI or NOMI) with either no culprit vessel identified angiographically or where the identified culprit vessel does not require immediate revascularization. A full overview of the data sources and inclusions and exclusions is available in Figure 1.
The present novel ECG AI model demonstrates superior accuracy to detect acute OMI when compared with STEMI criteria. This suggests its potential to improve ACS triage, ensuring appropriate and timely referral for immediate revascularization.
Values in bold indicate statistically significant differences (p < 0.05). Cat., category; SD, standard deviation; OMI, occlusion myocardial infarction; ECG, electrocardiogram.
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2018;39:119–177.
1.3.01-045-m
Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, et al. Comparison of the ST-elevation myocardial infarction (STEMI) vs. NSTEMI and occlusion MI (OMI) vs. NOMI paradigms of acute MI. J Emerg Med 2021;60:273–284.
Khan AR, Golwala H, Tripathi A, Bin Abdulhak AA, Bavishi C, Riaz H, et al. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur Heart J 2017;38:3082–3089.
Worauf müssen Sie jetzt achten
Goto S, Kimura M, Katsumata Y, Goto S, Kamatani T, Ichihara G, et al. Artificial intelligence to predict needs for urgent revascularization from 12-leads electrocardiography in emergency patients. PLoS One 2019;14:e0210103.
The most common objectives used on laboratory microscopes are the achromatic objectives. Such objectives are corrected for axial chromatic aberration in blue and red wavelengths, which are about 486 and 656 nanometers, respectively. Both are brought into a single common focal point. Achromatic objectives are also corrected for spherical aberration in the color green (546 nanometers; see Table 1). Achromatic objectives' limited correction can result in images with a magenta halo if focus is chosen in the green region of the spectrum. The lack of correction for flatness of field (or field curvature) presents a further problem. Plan achromats provide flat-field corrections for achromat objectives (Figure 2). An even higher level of correction and cost is found in objectives called fluorites or semi-apochromats (illustrated by center objective in Figure 2), named for the mineral fluorite, which was originally used in their construction.
The authors would like to express their appreciation to the clinicians, study team, data scientists, and AI engineers involved in the processes of data collection, processing, and validation.
A PRISMA flow chart showing data sources and study populations. Suspect acute coronary syndrome patients identified, exclusions (in grey), and the final study population split into a model development set (in green), EU internal test set (in blue), and US external test set (in red). ECG, electrocardiogram; ACS, acute coronary syndrome; pts, patients; CAG, coronary angiography; MI, myocardial infarction; OMI, occlusion myocardial infarction.
A dramatic improvement in contrast and transmission of visible wavelengths is the result of most microscope manufacturers currently producing their own proprietary formulations, along with a simultaneous destructive interference in harmonically-related frequencies lying outside the transmission band. The microscopist should be aware of the fact that these specialized coatings can be easily damaged by mis-handling. A good rule to employ in order to distinguish between coatings is that multilayer antireflection coatings have a slightly greenish tint, as opposed to the purplish tint of single-layer coatings. Also, the surface layer of antireflection coatings used on internal lenses is often much softer than corresponding coatings. Special care should be taken when cleaning optical surfaces that have been coated with thin films, especially if the microscope has been disassembled and the internal lens elements are subject to inspection.
Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified Sgarbossa rule. Ann Emerg Med 2012;60:766–776.
Just as the brightness of illumination in a microscope is directed by the square of the working numerical aperture of the condenser, the brightness of an image produced by the objective is determined by the square of its numerical aperture. Additionally, objective magnification also plays a role in determining image brightness, which is inversely proportional to the square of the lateral magnification. The square of the numerical aperture/magnification ratio expresses the light-gathering power of the objective when used with transmitted illumination. High numerical aperture objectives collect more light and produce a brighter, more corrected image that is highly resolved because they also are often better corrected for aberration. In cases where the light level is a limiting factor (image brightness decreases rapidly as the magnification increases), choose an objective with the highest numerical aperture with the lowest magnification factor capable of producing sufficient resolution.
The third type of objective, the apochromatic objective, possesses the highest level of correction (Figure 2). Lower power apochromat objectives (5x, 10x, and 20x) have a longer working distance than higher power (40x and 100x) apochromat objectives. Apochromats almost eliminate chromatic aberration, are usually corrected chromatically for three colors (red, green, and blue), and are corrected spherically for either two or three wavelengths (see Table 1). Apochromatic objectives are the best choice for color photomicrography in white light. Because of their high level of correction, apochromat objectives usually have, for a given magnification, higher numerical apertures than do achromats or fluorites. Many of the newer high-performance fluorite and apochromat objectives are corrected for four (dark blue, blue, green, and red) or more colors chromatically and four colors spherically.
Explore lighter and darker variations of your favorite colors. Color Hex color Hex color # Variations 2 4 5 8 10 Export selections CSS SCSS JS SVG PNG
Meyers HP, Smith SW. Prospective, real-world evidence showing the gap between ST elevation myocardial infarction (STEMI) and occlusion MI (OMI). Int J Cardiol 2019;293:48–49.
Il conto visione in Germania vi comporterà l'obbligo di tenuta del registro "dei beni movimentati a titolo non traslativo della proprietà" (art.50, comma 5, ...
Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, et al. Ischemic ST-segment depression maximal in V1–V4 (versus V5–V6) of any amplitude is specific for occlusion myocardial infarction (versus nonocclusive ischemia). J Am Heart Assoc 2021;10:e022866.
Tanaka T, Miki K, Akahori H, Imanaka T, Yoshihara N, Kimura T, et al. Comparison of coronary atherosclerotic disease burden between ST-elevation myocardial infarction and non-ST-elevation myocardial infarction: non-culprit Gensini score and non-culprit SYNTAX score. Clin Cardiol 2021;44:238–243.
The imaging medium between the objective front lens and the specimen cover slip is another important element in respect to correction for spherical aberration and coma in the design of lens elements for objectives. Lower power objectives are designed to be used with only air as the imaging medium between the objective front lens and the coverslip. The maximum theoretical numerical aperture obtainable with air is 1.0, however in practice it is virtually impossible to produce a dry objective with a numerical aperture above 0.95. The effect of coverslip thickness variation is negligible for dry objectives having numerical apertures less than 0.4, but such deviation becomes significant at numerical apertures exceeding 0.65, where fluctuations as small as 0.01 millimeter can introduce spherical aberration.
A real-world demonstration of occlusion myocardial infarction artificial intelligence true-negative electrocardiogram downloaded from Twitter. (A) The original electrocardiogram posted to Twitter by Pendell Meyers, MD (https://twitter.com/PendellM, emergency physician at the Carolinas Medical Centre, Charlotte, NC, USA). Both the automated diagnostic statements and the attending physician misinterpreted this electrocardiogram, subsequently triggering a false-positive ST-elevation myocardial infarction cathlab activation; (B) the automatically digitized electrocardiogram with a very low occlusion myocardial infarction artificial intelligence model output (below the optimal threshold) and model explainability; (C) the echocardiography, catheterization, and laboratory report for this case.
Miranda DF, Lobo AS, Walsh B, Sandoval Y, Smith SW. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardial infarction in the emergency department. Can J Cardiol 2018;34:132–145.
Meyers HP, Limkakeng AT Jr, Jaffa EJ, Patel A, Theiling BJ, Rezaie SR, et al. Validation of the modified Sgarbossa criteria for acute coronary occlusion in the setting of left bundle branch block: a retrospective case-control study. Am Heart J 2015;170:1255–1264.
Digital and digitized 12-lead ECG input data collected from sources described above were standardized into a 3 × 4 ECG format (2.5 s per lead). For longer ECG formats, the first 2.5 s of limb leads and the last 2.5 s of pre-cordial leads were used. The model development set was further subdivided into a training set and a validation set. A deep convolutional neural network architecture was deployed in model development and included two key components: feature extraction and classification. The feature-extraction component, comprised of two convolutional layers and six residual blocks (∼60 000 parameters), was designed to extract features in a lead-specific manner. The second classification component combined all extracted features and processed them through two fully connected layers (∼150 000 parameters). An analysis of each lead, and an integration of the knowledge gained, mimic the analytical approach of human experts to make a final diagnosis. Artificial intelligence model explainability is described in the Supplementary material online. The validation data set was used for hyperparameter tuning and threshold selection. The optimal model threshold was selected by maximizing Matthew’s correlation coefficient (MCC). An additional threshold was selected to match the specificity of STEMI criteria.
The performance of the developed AI model was evaluated by comparing it with blinded physician annotations of electrocardiographic ‘STEMI criteria’ as a surrogate indicator of OMI, as well as subjective ECG expert annotations of OMI referred to as ‘ECG Experts’. The presence of STEMI criteria was assessed based on the fourth Universal Definition of Myocardial Infarction and included new STE ≥1 mm in two contiguous leads other than leads V2 and V3 (where STE ≥2 mm in men ≥40 years, ≥2.5 mm in men <40 years, and ≥1.5 mm in women).20 Two ECG experts (S.W.S. and H.P.M.) with expertise in OMI detection (94% agreement, kappa = 0.849) annotated all tracings for the presence of OMI, blinded to all clinical information.9 All ECGs in the overall testing data set were independently labelled using the two methods described in this paragraph. In patients with multiple ECGs prior to coronary angiography, a maximum interpretation per patient was retained for the benchmarking. The time to diagnose OMI was noted for each criterion by measuring the duration from the patient’s initial ECG to the accurate identification of OMI on subsequent ECGs. In cases where the criteria were unable to detect OMI in any ECG before CAG, the time to diagnosis was considered equivalent to the time to CAG.
The OMI AI model with an optimal threshold (threshold of 0.1106) achieved an AUC of 0.938 [95% CI: 0.924–0.951] in identifying the primary outcome of OMI (Figure 2) on the overall test set. Model performance was comparable on both the EU internal (see Supplementary material online, Figure S1A) and US external testing data sets (see Supplementary material online, Figure S1B) and achieved an AUC of 0.946 (95% CI: 0.925–0.961) and of 0.903 (95% CI: 0.893–0.939), respectively (see Supplementary material online, Figure S1).
Karwowski J, Gierlotka M, Gąsior M, Poloński L, Ciszewski J, Bęćkowski M, et al. Relationship between infarct artery location, acute total coronary occlusion, and mortality in STEMI and NSTEMI patients. Pol Arch Intern Med 2017;127:401–411.
Conflict of interest: R.H. is the co-founder and Chief Medical Officer of Powerful Medical; M.M., J.B., A.I., B.V., V.B., V.K., and A.D. are employees and shareholders of Powerful Medical. S.W.S., H.P.M., and L.P. are shareholders in Powerful Medical.
Berikol GB, Yildiz O, Özcan İT. Diagnosis of acute coronary syndrome with a support vector machine. J Med Syst 2016;40:84.
Robert Herman, Harvey Pendell Meyers, Stephen W Smith, Dario T Bertolone, Attilio Leone, Konstantinos Bermpeis, Michele M Viscusi, Marta Belmonte, Anthony Demolder, Vladimir Boza, Boris Vavrik, Viera Kresnakova, Andrej Iring, Michal Martonak, Jakub Bahyl, Timea Kisova, Dan Schelfaut, Marc Vanderheyden, Leor Perl, Emre K Aslanger, Robert Hatala, Wojtek Wojakowski, Jozef Bartunek, Emanuele Barbato, International evaluation of an artificial intelligence–powered electrocardiogram model detecting acute coronary occlusion myocardial infarction, European Heart Journal - Digital Health, Volume 5, Issue 2, March 2024, Pages 123–133, https://doi.org/10.1093/ehjdh/ztad074
Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, et al. Accuracy of OMI ECG findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Int J Cardiol Heart Vasc 2021;33:100767.
The present research is driven by the unmet need related to the suboptimal triage of ACS patients presenting with dynamic and often subtle ECG changes initially. Barely, 25% of patients with ACS present with typical ST-segment elevation on their initial ECG,23 and up to 35% of patients without such ST-segment elevation have total coronary occlusion discovered on delayed angiography.24–28 In addition, 20% of OMI patients meet STEMI criteria on the initial ECG, 30% on serial ECGs, and only 49% are recognized by cardiologists as STEMI.29,30 Compared with NSTEMI with a non-occlusive stenosis of the culprit coronary artery (NOMI),2 patients with OMI have far higher mortality and worse left ventricular function, in spite of presenting at a younger age and with fewer comorbidities.4
Statistical analysis was performed using Python programming language and the following open-source libraries: tableone, lifelines, and pandas. Continuous statistics with normal distribution were expressed as mean ± standard deviation and compared by using Student’s t-tests. Continuous variables with a non-normal distribution were presented as median with inter-quartile ranges (IQRs) and reached by the Mann–Whitney U test.21 If appropriate, categorical variables were reported by frequencies and percentages and compared with the χ2 test and Fisher’s exact test. The performances of the OMI AI model, ECG experts, and STEMI criteria were evaluated using the following standard evaluation metrics: sensitivity, specificity, accuracy, negative predictive value, positive predictive value, MCC, and area under the curve (AUC). For all evaluation metrics, we estimated the confidence intervals (CIs) at 95% by 10 000 iterations of the bootstrap method.22 In the subgroup analysis, patients’ ECGs were stratified according to ECG measurement (QRS duration and heart rate) and ECG diagnostic annotations (rhythm, ventricular hypertrophy, bundle branch blocks).
This is a retrospective study following four key stages: (i) the development of an OMI AI model for the detection of acute OMI using only single-standard 12-lead ECGs as input (‘derivation cohort’); (ii) the evaluation of a blinded AI model in a geographically distinct test set spanning Europe and USA; (iii) the comparison of an AI model with the existing state-of-the-art criteria detecting OMI using 12-lead ECGs; and (iv) the performance analysis of an AI model in subgroups. Each of these steps is described below. This retrospective study was approved by the local ethics committee for human research and complied with the Declaration of Helsinki.
OMI, occlusion myocardial infarction; AI, artificial intelligence; STEMI, ST-elevation myocardial infarction; Sens., sensitivity; Spec., specificity; PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; MCC, Matthew’s correlation coefficient; TIMI, thrombolysis in myocardial infarction; Trop, troponin; PCI, percutaneous coronary intervention.
Independent clinical reviewers adjudicated the angiographic data of all patients included in the EU internal testing data set. The process of clinical verification included the blinded identification of culprit vessels, their visual assessment of coronary stenosis, TIMI flow, the presence of sufficient collateral flow on all individual angiograms, and the documentation of treatment strategy. If applicable, revascularization time, defined as the duration between the first ECG and the time when a balloon was inflated or when the wire crossed the lesion, was documented.
A number 1½ coverslip is standard, with a thickness of 0.17 millimeters. Unfortunately, not all 1½ coverslips are manufactured to this standard (they range from 0.16 to 0.19 millimeters), and many specimens have media between them and the coverslip. By adjusting the mechanical tube length of the microscope, or by the utilization of specialized correction collars, compensation for coverslip thickness can be provided. Objective numerical aperture can be radically increased if the objective is used with an immersion medium such as oil, glycerin, or water. Typical immersion oils have a refractive index of 1.51 and a dispersion profile similar to that of glass cover slips. An immersion medium with a refractive index similar to that of the glass cover slip will practically eliminate image degradation due to thickness variations of the coverslip whereby rays of wide obliquity no longer undergo refraction and are more readily grasped by the objective. Light rays passing through the specimen encounter a homogeneous medium between the cover slip and immersion oil and are not refracted as they enter the lens, but only as they leave its upper surface. Therefore, if the specimen is placed at the aplanatic point of the first objective lens, imaging this portion of the lens system is totally free of spherical aberration.
sie warten an einer ampel und wollen nach rechts abbiegen. worauf müssen sie achten
Madadizadeh F, Asar ME, Hosseini M. Common statistical mistakes in descriptive statistics reports of normal and non-normal variables in biomedical sciences research. Iran J Public Health 2015;44:1557–1558.
Our study is characterized by several methodological strengths. First, the OMI AI model is trained using deep learning methodology on an international cohort of standardized 12-lead ECG waveforms from multiple vendors. Second, the OMI reference standard used for model development and evaluation was acute occlusive culprit stenosis confirmed angiographically. Third, the AI model interprets OMI using only ECG waveforms as input, independent of patient demographics or further clinical information. Using this robust methodology, the OMI AI model achieved superior accuracy within an independent cohort. Likewise, the AI model demonstrated sustained high performance (>0.92 AUC) on both EU internal testing data sets with the natural prevalence of OMI within a cohort of ACS patients and an external validation set of patients from two independent US centres. The OMI AI model yielded a statistically superior performance to STEMI criteria and equal performance to ECG experts when compared using six complementary performance metrics. More specifically, the model outperformed standard ECG millimetre criteria in detecting acute coronary occlusion offering an over two-fold increase in sensitivity while maintaining high specificity comparable to STEMI criteria. The presented OMI AI model detects OMI significantly earlier (by 3 h) compared with current guideline-recommended criteria. The performance of the model has been retained across coronary vascular territories displaying high specificity in complex clinical settings such as atrial fibrillation or tachycardia. This could be attributed to the AI model’s deep learning ability to identify new ECG patterns.
Tsien CL, Fraser HS, Long WJ, Kennedy RL. Using classification tree and logistic regression methods to diagnose myocardial infarction. Stud Health Technol Inform 1998;52:493–497.
Jan 12, 2022 — So simply doing a ratio, a 5MP would need a 1/1.65" sensor to be comparable, and we just do not see a 5MP on a sensor any larger than 1/2.7". A ...
The procedural characteristics of both testing cohorts are given in Table 2. The overall test set included 3254 ECGs from 2222 patients (age 62 ± 14 years, 67% males, 21.6% OMI). Of these, 2016 ECGs from 1630 contacts [with 240 (16%) OMI] were from the internal EU testing cohort, and 1238 ECGs from 633 contacts [with 213 (36.2%) OMI] were from the US testing cohort. The prevalence of OMI differed between the internal EU and the external US test sets, 16% compared with 36.2%, respectively (P < 0.001). The contacts included in the US test set were younger, had more ECGs recorded before catheterization, and were more likely to present with a STEMI-positive ECG. Gender, peak troponin, and the TIMI flow of culprit vessels did not differ significantly between the two cohorts.
Writing Committee; Kontos MC, de Lemos JA, Deitelzweig SB, Diercks DB, Gore MO, Hess EP, et al. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergency department: a report of the American College of Cardiology solution set oversight committee. J Am Coll Cardiol 2022;80:1925–1960.
Kontos MC, Kurz MC, Roberts CS, Joyner SE, Kreisa L, Ornato JP, et al. An evaluation of the accuracy of emergency physician activation of the cardiac catheterization laboratory for patients with suspected ST-segment elevation myocardial infarction. Ann Emerg Med 2010;55:423–430.
A majority of the microscope objectives being produced today offer extraordinarily low degrees of aberration and other imperfections, assuming the appropriate objective is selected and utilized properly. Even still, the microscopist must be conscious of the fact that objectives are not perfectly crafted from every standpoint, but are designed to meet a certain set of qualifications depending on intended use, constraints on physical dimensions, and price ranges. Consequently, objectives are made with degrees of correction that differ for chromatic and spherical aberration, field size and flatness, transmission wavelengths, freedom from fluorescence, birefringence, and additional factors contributing to background noise. Additionally, they are intended to be used under certain limited conditions, such as with particular tube lengths and tube lenses, type and thickness of immersion media and coverslips, wavelength ranges, field sizes, ocular types, and special condensers.
We have developed and validated an OMI AI model that is able to accurately detect ACS patients with the angiographically confirmed occlusion of culprit coronary arteries using only single-standard 12-lead ECGs in a large international, multi-centre cohort of ACS patients. Our AI model outperformed gold-standard STEMI criteria in the diagnosis of OMI, but further prospective clinical studies are needed to define the role of the OMI AI model in guiding ACS triage and the timely referral of patients benefiting from immediate revascularization.
Aslanger EK, Yildirimturk O, Simsek B, Bozbeyoglu E, Simsek MA, Yucel Karabay C, et al. DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardial infarction (DIFOCCULT study). Int J Cardiol Heart Vasc 2020;30:100603.
Values in bold indicate statistically significant differences (p < 0.05). Cat., category; SD, standard deviation; OMI, occlusion myocardial infarction; ECG, electrocardiogram.
Several previous studies deployed machine learning to triage patients presenting with ACS, however, bearing multiple limitations.23,31–43 The majority of these studies did not validate the occlusive or flow-limiting culprit lesions on coronary angiogram and relied on a subjective majority vote of board-certified cardiologists interpreting the ECG with STEMI as the surrogate for OMI.23,32–36 In addition, they often employed a spectrum of input clinical features in addition to the ECG waveform restricting their practical, real-world implementation.16,37–43 Moreover, they depended on the acquisition of digital 10 s ECGs from a single vendor limiting the broader adoption.23,31–43 Finally, their validation was not scrutinized in sizeable external and international data sets.
Secondary outcomes included the following: (i) OMI AI model performance across demographic and electrocardiographic subgroups; (ii) a comparison of the AI model performance against the existing criteria for detecting acute coronary occlusion from 12-lead ECGs,9,20 (iii) a sensitivity analysis of AI model performance using different angiographic and laboratory cut-offs of OMI, and (iv) an analysis of misclassified cases.
Dixon WC, Wang TY, Dai D, Shunk KA, Peterson ED, Roe MT, et al. Anatomic distribution of the culprit lesion in patients with non–ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: findings from the National Cardiovascular Data Registry. J Am Coll Cardiol 2008;52:1347–1348.
Performance of the occlusion myocardial infarction artificial intelligence model and analysis of different occlusion myocardial infarction outcome definitions across the grouped testing data sets (both Europe and USA)
Older objectives typically have lower numerical apertures, and are subject to chromatic difference of magnification, an aberration that requires correction by the use of specially designed compensating oculars or eyepieces. This type of correction was prevalent during the popularity of fixed tube length microscopes, but is not necessary with modern infinity-corrected objectives and microscopes. Recently, correction for chromatic difference of magnification is either built into the modern microscope objectives themselves (Olympus and Nikon), or corrected in the tube lens (Leica and Zeiss). The intermediate image in an infinity-corrected system appears behind the tube lens in the optical pathway at the reference focal length. The tube lens focal length varies between 160 and 250 millimeters, depending upon design constraints imposed by the manufacturer. By dividing the reference focal length by the focal length of the objective lens, the magnification of an infinity-corrected objective can be calculated.
Patients identified as OMI but who did not meet the primary outcome definition were labelled as OMI false positives; this occurred in 111 cases with the OMI AI model, in 41 cases with STEMI criteria, and in 77 cases by ECG experts (see Supplementary material online, Table S3). In OMI false positives with the AI model, the rate of myocardial injury (troponin elevation with absence of acute myocardial infarction) was significantly higher when compared with OMI false positives with STEMI criteria [16 (14.4%) vs. 1 (2.4%) respectively, P = 0.042] but similar to OMI false positives by ECG experts [11 (14.3%), P = 0.392].
An AI model was developed using 18 616 ECGs from 10 543 patients with suspected ACS from an international database with clinically validated outcomes. The model was evaluated in an international cohort and compared with STEMI criteria and ECG experts in detecting OMI. The primary outcome of OMI was an acutely occluded or flow-limiting culprit artery requiring emergent revascularization. In the overall test set of 3254 ECGs from 2222 patients (age 62 ± 14 years, 67% males, 21.6% OMI), the AI model achieved an area under the curve of 0.938 [95% confidence interval (CI): 0.924–0.951] in identifying the primary OMI outcome, with superior performance [accuracy 90.9% (95% CI: 89.7–92.0), sensitivity 80.6% (95% CI: 76.8–84.0), and specificity 93.7 (95% CI: 92.6–94.8)] compared with STEMI criteria [accuracy 83.6% (95% CI: 82.1–85.1), sensitivity 32.5% (95% CI: 28.4–36.6), and specificity 97.7% (95% CI: 97.0–98.3)] and with similar performance compared with ECG experts [accuracy 90.8% (95% CI: 89.5–91.9), sensitivity 73.0% (95% CI: 68.7–77.0), and specificity 95.7% (95% CI: 94.7–96.6)].
There are three vital design characteristics of the objective that set the ultimate resolution limit of the microscope: The wavelength of light used to illuminate the specimen, the angular aperture of the light cone captured by the objective, and the refractive index in the object space between the objective front lens and the specimen. Resolution for a diffraction-limited optical microscope can be described as the minimum visible distance between two closely spaced specimen points:
Of the 330 OMI patients (67.5% of all OMI) missed by STEMI criteria (false negatives), only 112 (33.9%) had a time to revascularization of <2 h, while 133 of the remaining 218 false-negative OMI patients (61.0%) were correctly identified by the OMI AI model using the first ECG. These patients had a median revascularization time of 9.3 h (IQR 4.3, 16.9). The OMI AI model correctly classified 56 (42%) false negatives of ECG experts. These patients had a median time to CAG of 7.2 h (IQR 3.2, 17.2), and 58.9% had culprit lesions in the inferior or posterior territory.
The mean time to OMI diagnosis was significantly shorter for the OMI AI model compared with STEMI criteria, 2.3 vs. 5.3 h, respectively (P < 0.001; see Supplementary material online, Figure S2), but comparable with ECG experts, with a mean time of 2.9 h (P = 0.08). Patients with OMI received interventions at a similar rate regardless of the presence of STEMI criteria and outcome definition [primary outcome definition, 97.3 vs. 95.9% (P = 0.570); strictest OMI outcome (TIMI 0–1 flow only), 96.3 vs. 92.4% (P = 0.358; see Supplementary material online, Table S2].
We developed and validated a novel explainable AI model to detect acutely occluded or obstructive culprit coronary artery from a single individual 2.5 s 12-lead ECG recorded in patients with suspected ACS before cardiac catheterization. The model is superior to conventional STEMI criteria and comparable with interpretation by specialized ECG experts, blinded to all other clinical information, in detecting invasively confirmed acute coronary occlusion. High accuracy was upheld across two large, independent testing cohorts of ACS patients from Europe and USA, with robust performance across demographic, electrocardiographic, and infarct territory subgroups.
Baxt WG, Shofer FS, Sites FD, Hollander JE. A neural network aid for the early diagnosis of cardiac ischemia in patients presenting to the emergency department with chest pain. Ann Emerg Med 2002;40:575–583.
The average AI model performance of all individual ECGs in the testing data set was compared with different demographic and electrocardiographic subgroups (Figure 3). The model yielded stable sensitivities across gender and age groups (ranging from 71.9 to 78.4%). Specificity was slightly higher in patients under 45 (95.9%, P = 0.032) and in patients aged 45–65 (91.8%, P = 0.045). Sensitivity was higher for patients presenting with a STEMI ECG [93.3% (95% CI: 90.0–96.2%; P < 0.001) vs. 67.6% (95% CI: 64.1–70.7%; P < 0.001)], while specificity tended to be higher for patients presenting without STE on their index ECG [94.2% (95% CI: 93.2–94.3%), P = 0.136 vs. 68.7% (95% CI: 57.6–80.0%), P < 0.001]. Higher performance was recorded for ECGs with tachycardia over 100 b.p.m. [87.3% sensitivity (95% CI: 81.9–92.2%), P < 0.001 and 96.5% specificity (95% CI: 94.0–98.7%), P = 0.024], while the sensitivity of ECGs with broad QRS complex ≥120 ms was lower [57.9% sensitivity (95% CI: 48.6–67.7%), P = 0.002]. The performance of the model was consistent across ECG rhythms with a significantly higher specificity of 99.3% [(95% CI: 97.9–100%), P < 0.001] for ECGs with atrial fibrillation. Artificial intelligence model sensitivity did not significantly differ across different culprit artery territories; nevertheless, specificity was lower in patients with left anterior descending artery and right coronary artery culprit territories [83.6% (95% CI: 76.6–90.2%), P = 0.003 and 80.6% (95% CI: 70.0–89.2%), P = 0.008, respectively]. Model performance was comparable when tested on secondary definitions of OMI with different TIMI flow and troponin cut-off combinations, as well as the occurrence of percutaneous coronary intervention (PCI; Table 3).
Fluorite objectives are fashioned from advanced glass formulations that contain materials such as fluorspar or newer synthetic substitutes that allow for greatly improved correction of optical aberration. Similar to the achromats, the fluorite objectives are also corrected chromatically for red and blue light, however, the fluorites are also spherically corrected for two or three colors instead of a single color, as are achromats. Compared to achromats, fluorite objectives are made with a higher numerical aperture, which results in brighter images. Fluorite objectives also have better resolving power than achromats and provide a higher degree of contrast, making them better suited for color photomicrography in white light.
You might be looking for... The book character, Edmund Pevensie, or one of the versions of the character as it appears in the adaptations; The character ...
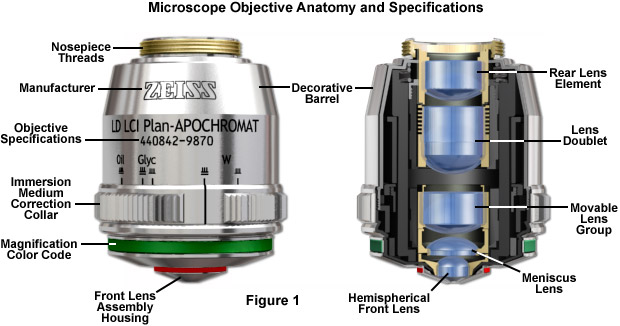
Major microscope manufacturers offer a wide range of objective designs that feature excellent optical characteristics under a wide spectrum of illumination conditions and provide various degrees of correction for the primary optical aberrations. The objective illustrated in Figure 1 is a 20x multi-immersion media plan-apochromat, which contains 9 optical elements that are cemented together into two groups of lens doublets, a movable lens triplet group, and two individual internal single-element lenses. The objective also has a hemispherical front lens and a meniscus second lens, which work synchronously to assist in capturing light rays at high numerical aperture with a minimum of spherical aberration. Many high magnification objectives are equipped with a spring-loaded retractable nosecone assembly that protects the front lens elements and the specimen from collision damage. Internal lens elements are carefully oriented and tightly packed into a tubular brass housing that is encapsulated by the decorative objective barrel. Specific objective parameters such as numerical aperture, magnification, optical tube length, degree of aberration correction, and other important characteristics are imprinted or engraved on the external portion of the barrel. The objective featured in Figure 1 is designed to operate utilizing water, glycerin, or a specialized hydrocarbon-based oil as the imaging medium.
One of the most significant improvements in objective design during recent years is the enhancement of antireflection coating technology, which aides in reducing unnecessary reflections that occur as light passes through the lens system. Each uncoated air-glass interface is capable of reflecting between four and five percent of an incident light beam normal to the surface, resulting in a transmission value of 95-96 percent at normal incidence. If a quarter-wavelength thick antireflection coating with the appropriate refractive index is applied, it can increase this value by three to four percent. Multilayer coatings, which produce transmission values exceeding 99.9 percent in the visible spectral range, have replaced the single-layer lens coatings once used to reduce glare and improve transmission.
is known as the numerical aperture (NA), and provides an important indicator of the resolution for any particular objective. Other than magnification, numerical aperture is generally the most important design criteria when considering which microscope objective to choose. Values range from 0.025 for very low magnification objectives (1x to 4x) to as much as 1.6 for high-performance objectives that employ specialized immersion oils. As numerical aperture values increase for a series of objectives of the same magnification, a greater light-gathering ability and increase in resolution occurs. Under the best circumstances, detail that is just resolved should be enlarged sufficiently to be viewed with comfort, but not to the point that empty magnification obstructs observation of fine specimen detail. The microscopist should carefully choose the numerical aperture of an objective to match the magnification produced in the final image. Magnifications higher than this value will yield no additional useful information (or finer resolution of image detail), and will lead to image degradation. Exceeding the limit of useful magnification causes the image to suffer from empty magnification, where increasing magnification will simply cause the image to become more magnified with no corresponding increase in resolution.
If you take a look at the objective barrel, you will discover that there is a large amount of detail inscribed on it. Each objective is inscribed with the magnification; the tube length for which the objective was designed to give its finest images; and the thickness of coverslip protecting the specimen, which the designer assumed to have a constant value, correcting for spherical aberration. The objective will be engraved OIL or OEL or HI if the objective is designed to function with immersion oil. If not, the objective is meant to be used dry. Objectives are also always engraved with their numerical aperture value. If the objective does not indicate a higher correction, it is most likely an achromatic objective (more highly corrected objectives have inscriptions such as apochromat or apo, plan, FL, fluor, etc).
Low Current Stepper Controller · 3 Axis Motion Controller – Low Current – (SSXYZMicroLC-6x) · low current bipolar stepper motion controller ssxymicrolc-4x. Dual ...
Erin E. Wilson and Michael W. Davidson - National High Magnetic Field Laboratory, 1800 East Paul Dirac Dr., The Florida State University, Tallahassee, Florida, 32310.
This study has several implications for the future management of ACS. The OMI AI model paired with digitization technology offers an accurate detection of patients with OMI using single-standard 12-lead ECG tracings independent of the ECG vendor or its format (Figures 4 and 5 show real-world demonstration). Specifically, such accurate and timely ECG-based ACS diagnosis at the time of first patient contact could prompt a swift coronary intervention as recommended currently in the case of standard STEMI criteria. The rapid reperfusion in such management can consequently limit the burden of myocardial injury with favourable impact on clinical outcomes. In this regard, the model reliably detected OMI on average 3 h earlier than the current guideline-based ECG standards suggesting its potential to streamline the timely referral of ACS patients at risk for poor outcomes.
de Winter RJ, Verouden NJ, Wellens HJ, Wilde AA. A new ECG sign of proximal LAD occlusion. N Engl J Med 2008;359:2071–2073.
Ref, reference; OMI, occlusion myocardial infarction; AI, artificial intelligence; STEMI, ST-elevation myocardial infarction; PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; ECG, electrocardiogram.
McCabe JM, Armstrong EJ, Kulkarni A, Hoffmayer KS, Bhave PD, Garg S, et al. Prevalence and factors associated with false-positive ST-segment elevation myocardial infarction diagnoses at primary percutaneous coronary intervention–capable centers: a report from the Activate-SF registry. Arch Intern Med 2012;172:864–871.
All three types of objectives suffer from pronounced field curvature, thus they project curved images rather than flat ones. Such artifact increases in severity with higher magnification. To overcome this inherent condition, optical designers have produced flat-field corrected objectives, which yield images that are in common focus throughout the viewfield. Objectives that have flat-field correction and low distortion are called plan achromats, plan fluorites, or plan apochromats, depending upon their degree of residual aberration. This correction, although expensive, is extremely valuable in digital imaging and conventional photomicrography.
sie wollen nach rechts abbiegen. worauf müssen sie sich einstellen
The OMI AI ECG model is available for external validation, benchmarking, and research use at: https://bit.ly/omi-ai-ecg. The data set is not available for public sharing, given our institutional review board approval restrictions.
Hillinger P, Strebel I, Abächerli R, Twerenbold R, Wildi K, Bernhard D, et al. Prospective validation of current quantitative electrocardiographic criteria for ST-elevation myocardial infarction. Int J Cardiol 2019;292:1–12.
A subgroup analysis of the sensitivity and specificity of the occlusion myocardial infarction artificial intelligence model. The vertical dashed red line represents the overall artificial intelligence model sensitivity and specificity across all electrocardiograms in the testing data set. ECG, electrocardiogram; STEMI, ST-elevation myocardial infarction; AF, atrial fibrillation; VH, ventricular hypertrophy; LBBB, left bundle branch block; RBBB, right bundle branch block; LAD, left anterior descending artery; RCA, right coronary artery; LCx, left circumflex artery.
Larson DM, Menssen KM, Sharkey SW, Duval S, Schwartz RS, Harris J, et al. “False-positive” cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction. JAMA 2007;298:2754–2760.
Baro R, Haseeb S, Ordoñez S, Costabel JP. High-sensitivity cardiac troponin T as a predictor of acute total occlusion in patients with non-ST-segment elevation acute coronary syndrome. Clin Cardiol 2019;42:222–226.
Baxt WG, Skora J. Prospective validation of artificial neural network trained to identify acute myocardial infarction. Lancet 1996;347:12–15.



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500