
The Mathematics of Lenses - how to find the magnification of a lens
Collimator
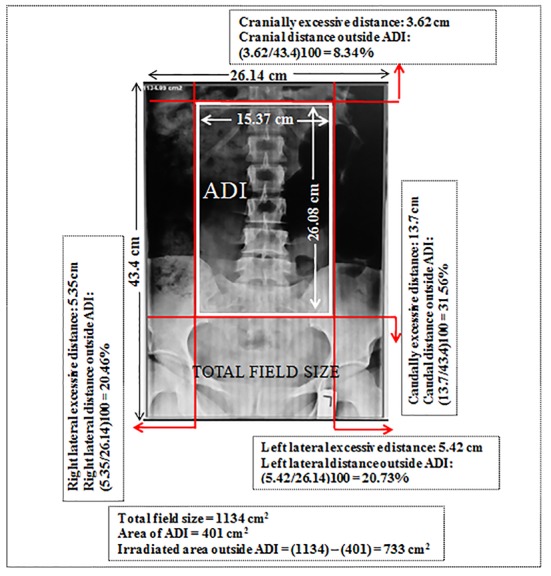
Distance outside ADI of each side (%) = [(Distance between current and optimal collimation of each side) / (Distance of current collimation)] × 100 (2)
Learn what a bandpass filter is and the features that should be considered when designing a bandpass filter. Omega can design and manufacture a custom filter that will differentiate your product.
How to collimate a divergingbeamof light
In order to minimize such risks and concerns, it is essential to decrease the received doses as low as reasonably achievable (ALARA); hence, all possible radiation dose reduction methods must be employed [6]. Collimating the primary beam to the area of diagnostic interest (ADI) has been strongly recommended as an effective method to reduce patient’s radiation dose and to increase image quality in radiology practice [6-9]. Proper collimation reduces the amount of tissue irradiated and the following radiation risk. Increasing image quality by reducing scatter radiation is an added benefit when using collimation [6,8].
Articles from Journal of Biomedical Physics & Engineering are provided here courtesy of Shiraz University of Medical Sciences
Omega cannot guarantee availability of displayed products. Contact us for details, or to request pricing of a custom part.
One of the common reasons to apply larger collimation by radiographers is the fear of cutting the ADI and the attitude that it is better to be larger than cutting of the ADI and/or repetition of the examination. An appropriate solution is learning to use anatomical landmarks for collimation guide. Adequate collimation during spine radiography is required to understand these surface anatomical landmarks associated with various vertebral segments that can be easily palpated. The most reliable landmarks for collimation guide are shown in Table 2. It is note that it should serve as the only point of departure for radiographers toward orientation since considerable individual variation will be encountered in daily practice. This study only evaluated the status of collimation during lumbar spine radiography. Other directions of future studies can evaluate the length status of the field of scan during computerized tomography (CT) examinations. It is significant since the doses from CT are 100-500 times more than conventional radiography [22].
Collimatedbeammeaning
21 Omega Drive Brattleboro, VT 05301 USA U.S. Toll-Free: 1-866-488-1064 International: +1 (802) 251-7300 Sales and Support: sales@omegafilters.com Press: marketing@omegafilters.com
The results of this study emphasize the fact that patients receive avoidable excessive radiation dose due to large collimation. Based on our results, at least in 62/5% of radiographs evaluated, ovaries were included in the primary beam while they were not of interest. As known from literature [19-21], a significant dose reduction can be achieved by using gonadal shield, of 830 radiographs under investigation; we found that only one radiograph had an evidence of gonad shielding. However, discussion on gonad protection is not the focus of this study.
Laserbeam collimation
*Corresponding author:M. Zabihzadeh, PhD, Assistant professor, Department of Medical Physics, School of Medicine, Ahvaz Jundishapur University of Medical Sciences, Golestan Blvd., Ahvaz, Iran
Collimationradiology
This study evaluated the quality of beam collimation during lumbar spine radiography. Transition from analogue to digital radiography has increased concerns in terms of neglecting proper collimation. Two primary concerns are the digital image receptors are more sensitive to the low levels of radiation produced due to the large collimation, which causes a reduction in image contrast [14], and also electronic masking or cropping of digital images to the ADI may be a reason to become complacent of radiographers toward proper collimation [9,14]. These concerns have led to several published studies [9,10,15]. Zetterberg and Espeland (2011) conducted a study to examine the quality of beam collimation in 86 analogues and 86 digital lumbar spine radiographs, and reported that the mean total field size was 46% larger in digital than in analogue images. They highlighted these larger irradiated areas as causing unnecessary high radiation doses to patients [9]. Debess et al. (2015) evaluated collimation in 186 chest radiographs and reported that 76% to 90% of the evaluated radiographs had large collimations [10]. A survey of 450 radiographers by the American Society of Radiologic Technologists (ASRT) revealed that half of the respondents used electronic cropping after the exposure [15].
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Collimating lens vs focusing lens
After approval, we retrospectively reviewed the digital image library of two general hospitals of Ahvaz, Iran to identify the patients who underwent lumbar spine radiography during five last months (from 21 April to 23 August 2015). Images were considered eligible for inclusion if patient’s age was over 16 years old and not taken to scoliosis. In general, 830 antero-posterior (AP) lumbar spine radiographs (574 in hospital A and 256 in hospital B) of 503 male and 327 female were obtained. All radiographs were retrospectively reviewed in terms of beam collimation. In order to achieve consistency, all radiographs were reviewed by a single person. The criteria for adequately collimation were based on available standard protocols [9,11-13]. According to this protocol, x-ray beam should be collimated on four sides of the lumbar spine as a cranial limit to the upper border of 12th thoracic vertebra, caudally to the lower border of 1th sacrum vertebra and laterally on each side by a vertical line at the lateral border of the sacroiliac joints. The distance between current and optimal collimation of each radiograph was calculated (in cm) using exact electronic ruler available at workstation monitors. The ADI and total irradiated area (the applied field size) for each radiograph was also electronically calculated (in cm2) (Figure 1). Irradiated region outside ADI and the percentage distance outside ADI from each side for each radiograph were also calculated by equations as:
The results of this study reveal that all radiographs evaluated more and less had large collimations, as the total irradiated field size outside ADI was 1.26 times more than ADI. Previous studies that evaluated the lumbar spine radiographs [9] and chest radiographs [10] found also larger collimation than acceptable. The results of this study also are in contrast to Rahimi et al. [16] in which the collimation of primary beam to the ADI during general radiography was reported 46.4%.
Inadequate collimation has been identified as the largest contributor and the most frequent cause of unnecessary patient’s radiation dose [7]. As reported by Dowd and Tilson, reducing field size from 8×10 to 6×6 inch results in 50% reduction in absorbed radiation dose to the patient during lumbar spine radiography [6]. Doubling the primary beam region results in doubling integral patient dose [7]. A significant increase of 25% radiation dose to the stomach (a point at distance of 10.2 cm from the field edge) has also been reported during chest radiography following the use of improper large collimation [10]. Lack or inadequate collimation of x-ray beam to the ADI during lumbar spine radiography is associated with excessive radiation dose to the surrounding critical organs (gonads, breast and colon) and deterioration of image quality. Therefore, it is essential that we limit the field size strictly to the ADI.
The total mean ADI and irradiated region outside ADI for each radiograph were estimated 360 and 454 cm2, respectively. The total irradiated region outside ADI was 1.26 times more than ADI. In contrast to cranial regions outside ADI, caudal regions were more commonly included inside the primary beam (12% vs. 24.4%; P-value <0.005). At least in 62% of radiographs evaluated, ovaries were included in the primary beam.
Conventional radiological procedures are a significant source of radiation exposure to the population, and its use has increased substantially over the past decades [1,2]. Among all conventional radiographic examinations, lumbar spine radiography is associated with the highest radiation dose [3], as it is responsible for the highest collective dose to the UK population [4]. Locating the most radiosensitive organs such as gonads, breast and colon (with high tissue weighting factors of 0.08, 0.12 and 0.12, respectively [5]) in or near the primary radiation field during radiography of the lumbar spine, raises concerns about patient’s safety [3,4].
Collimating lens
Radiographers should make considerable effort to limit the primary beam to the ADI to reduce patient’s exposure and to increase image quality.
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
How to make a collimatedbeam
Our results demonstrated that patients in hospitals investigated received excessive radiation doses due to large collimation. Improper radiation collimation causes unnecessarily high radiation doses to patients which should be reversed. Radiographers should make considerable effort to limit the primary beam to the ADI to reduce patient’s exposure and to increase image quality, simultaneously. The provision of written collimation guidelines in radiography rooms and its practical training are also recommended.
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
Collimating the primary beam to the area of diagnostic interest (ADI) has been strongly recommended as an effective method to reduce patient’s radiation dose and to improve image quality during radiology practice. Lack or inadequate collimation results in excessive radiation dose to patients and deterioration image quality.
A Monte Carlo study by Chaparian et al. (2014) revealed that the mean radiation absorbed doses to the colon, breast, ovaries and testicles from only AP projection of the lumbar spine radiography were 0.902, 0.014, 0.613 and 0.429 mSv, respectively [17]. Following this, the mean risk of radiation-induced fatal cancer for males and females has also been estimated 18.55 and 17.50 per million, respectively [17]. These values certainly simulated the assumption of good collimation and proper alignment of x-ray field with appropriate anatomical landmarks; therefore, it can substantially increase if these organs are included in the primary beam due to large collimation. Although excessive radiation dose produced by large collimation may not be significant, due to frequency of examinations (LS radiography has been identified as the third mostly frequent radiographic procedure performed [18]) and the use of various views (six views for individual person in the same area), the cumulative radiation dose could be significant. As reported by Vader et al. (2004), a number of 273,000 lumbar spine radiographies are performed annually in Switzerland which is responsible for 1130 Sv collective radiation dose to the population [18].
We retrospectively reviewed 830 digital antero-posterior (AP) lumbar spine radiographs in term of beam collimation. For each radiograph, the distance between current and optimal collimation was calculated (in cm). The area of ADI and total field size for each radiograph were also calculated (in cm2).
The total mean ADI and irradiated region outside ADI for each radiograph were estimated 360 and 454 cm2, respectively. The total irradiated region outside ADI was 1.26 times more than the ADI. In contrast to cranial regions outside ADI, caudal regions were more commonly included inside the primary beam (12% vs. 24.4%; P-value <0.005) (Table 1). At least in 62% of radiographs evaluated, ovaries were included in the primary beam. In addition, in terms of proper collimation, we found no significantly statistical differences between two inspected hospitals (P-value > 0.005) and also between male and female patients (P-value > 0.005).



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500