
Quantum and Interband Cascade Lasers (QCLs and ICLs), 3 - laser cascade
Severity of visual loss, depends upon the distance of the laser impact site from the centre of the fovea, the extent of the chorioretinal disruption and amount of chorioretinal bleed.1,2,3,4,5 Rapid tissue expansion or distortion caused by extremely high irradiances during short exposure can result in retinal, subhyaloid, subretinal and or choroidal hemorrhages that cause temporary visual deficit if involving the central fundus. These deficits were present in Cases number 1 and 2 in our series.3,4,5,6 Permanent visual deficit occurs if there is an underlying damage to the retinal structure.5,6,7,8 For example Case number 1 had persistent poor vision due to alteration of retinal structure noted on optical coherence tomography. In Case number 2, the final visual outcome remains unknown as patient was lost to follow up.
Retinal injuries due to laser pointers or devices have legal, financial and medical consequences. Most accidents are prevented by natural reflexive protective mechanisms.4,5,6 A lack of information on the types of lasers and the hazards, mis-information or lack of information to consumers, by laser device manufacturers, easy availability of hazardous lasers that resemble safe lasers are a few of the factors that can lead to careless use.1,2,3,4,5,6,7 Strict legislation, prohibiting the manufacture, use or possession of hazardous laser pointers, public education and education of the military sector about the hazards of lasers is mandatory, especially due to increased use of lasers for military applications.1,2,3,4,5,6,7,8,9,10
Circular PolarizerFilm
Two young soldiers (Cases 1 and 2) aged 27 and 28 years respectively, serving in the Oman army, projected penlight like devices emanating bright blue-green light into each others eyes (left eye for Case number 1 and right eye for Case number 2) for about 5–10 s. They competing with each other to determine who could bear the light longer while celebrating the success of a local football game. Both individuals experienced some after images, severe photophobia and headache followed by blurred vision the next day.
Suffers from a quarter-century and counting film and manual focus SLR addiction. Has recently expanded into 1980's AF point and shoots, and (gack!) '90s SLRs. He even mixes in some digital. Definitely a sick man.
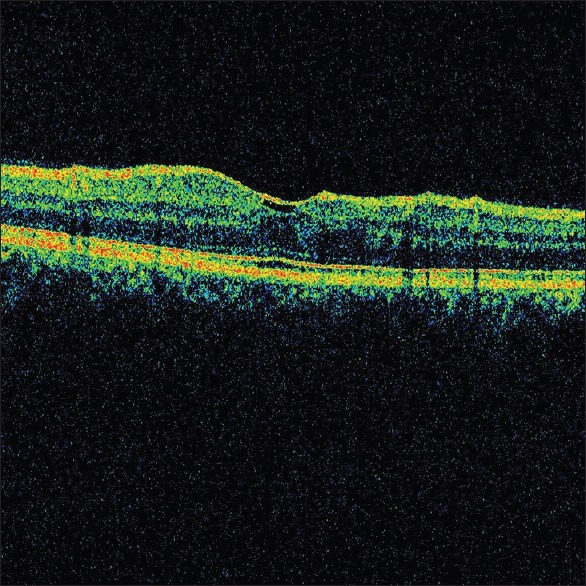
(a) Optical coherence tomography OD - normal macula. (b) Optical coherence tomography OS - showing shadowing of macula by subhyaloid hemorrhage, horizontal level and sup macula seen, ILM irregular
Corresponding Author: Dr. Radha Shenoy, Department of Ophthalmology, Armed Forces Hospital, Muscat, Sultanate of Oman. E-mail: shenoyvss@gmail.com
(a) Optical coherence tomography macula OD - shadowing due to subhyaloid haemorrhage. (b) Optical coherence tomography macula OS - normal
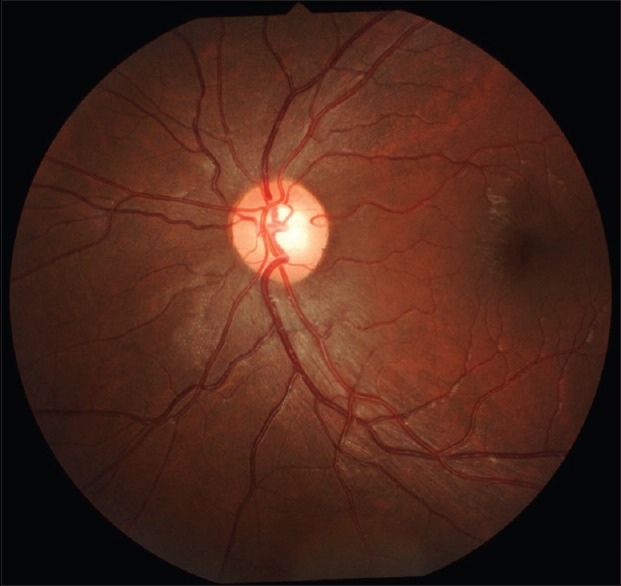
(a) Fundus photograph of normal OD. (b) Fundus photograph OS showing subhyaloid hemorrhage at the posterior pole with horizontal level
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Linearvscircular polarizerreddit
Allen et al.2 reported full thickness foveal hole in a 20-year-old man due to accidental exposure from a hand held Nd: YAG laser range finder device. Presence of strong reflections from the choroid underlying the hole on optical coherence tomogram, lead the authors to study the injury pattern by experimentally producing laser induced macular holes in non human primate models. They noted that this specific type of laser induced trauma required a minimum total intraocular energy of about 1–3 mJ.2,3,4 Laser induced macular holes were similar to idiopathic macular holes clinically and on angiography, but differed on optical coherence tomography, in that the former had increased reflectivity at the base due to scarring of the underlying choroid, similar to Case 3 in our series.1
The output of laser pointers available to the general public is limited and varies by country.6,7,8,9,10 As per the United States Food and Drug Administration Code of Federal Regulations, “demonstration laser products” like pointers must comply with applicable requirements for Class I, IIa, II, or IIIa devices.1,2,3,4,5,6,7,8,9,10
BestCircular polarizer
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Excellent info on polarizers: for years I used a linear with an OM-4. Just purchased my 2nd OM-4, and was going to pick up with the linear again until I read this. Too much info out there that AF is the only determining factor: not enough info about exposure systems.
Case 3 was another soldier who was 28 years old and presented approximately 8–9 months after presentation of Cases 1 and 2 with a similar history. However, he reported to the clinic immediately after exposure. On examination, best corrected visual acuity was 6/5 with a refraction of −0.25 D sphere in the right eye and 1/60 with a refraction of −0.25 D sphere in the left eye with no improvement on pinhole testing. Amsler grid testing indicated normal results in the right eye and a central scotoma in the left eye. On fundus evaluation the CDRs were 0.3 bilaterally, the retinal vessels and fovea in the right eye were normal. There was a well circumscribed round hole at the fovea in the left eye [Figure 10]. On Optical coherence tomography, the macula was normal in the right eye, and there was a full thickness macular hole with cystoid changes at the edges of the hole and increased reflectivity at the base in the left eye [Figure 11]. Fluorescein angiography of the right eye was unremarkable and there was a window defect in the left eye corresponding to the full thickness macular hole [Figure 12].
Recently unregulated lasers have been imported in the Middle East and can be easily acquired by the public here, we present three cases of military personnel with unilateral visual loss and retinal lesions following alleged exposure to laser pointers. None of the individuals were aware that the bright blue-green light projected into their eyes was from a laser pointer and was harmful.
Linear polarizervscircular polarizerphotography
Class 2 lasers cause damage to retina if the beam is viewed for more than 10 s at close range. Class 3 lasers, especially 3R and 3B are hazardous and prohibited in many countries but are easily available online and are popular with teenagers.7 Class 4 lasers are the most powerful lasers, and are used in military and occupational settings, such as laser shows. They are capable of producing extensive ocular damage.4,5,6,7,8,9,10
Nd: YAG laser hyaloidotomy is a safe and effective procedure, achieving rapid resolution of premacular subhyaloid haemorrhage with restoration of visual function while preventing the need for vitreoretinal surgery.8 In our case series, treatment was declined by Case number 1 and ineffective in Case number 2.
(a) Fundus fluorescein angiography OD - normal dye transit. (b) Fundus Fluorescein angiography OS - showing hyperfluorescence at the site of full thickness macular hole
Laser pointers are practical and safe training tools when used properly. If used incorrectly they can cause ocular damage, potentially resulting in devastating vision loss. The ocular and visual morbidity can result in significant expenses for medical care and inability to work (temporarily or permanently) for civilians and military personnel. We present three cases of soldiers who experienced vision loss following exposure to laser pointers, while celebrating successfull football game.
Circularvslinear polarizerfor mirrorless camera
Glad to hear that you found the article helpful. I must confess that I never gave much thought to the metering side of things until I researched why they came up with circular polarizers in the first place during the 1960s...due to Leica and Canon pioneering the use of beam splitters for their SLR exposure meters. Best regards.
The following Ophthalmologists and Optometrists have supported us in the collection of data that has aided in the preparation of this manuscript and we acknowledge their support, without which this manuscript would not have been complete. Dr. Milind Suryavanshi M.S (Ophth) Diplomate. FRCS (Glas), Dr. Santhosh K Philip M.S. (Ophth), Dr. Rashid Mohammed Al Saedi M.D. FEBO, Dr. Badar Mohammed Al Barwani MBChB (Glas). F.R.C.S. (Edin) and Optometrists Mr. Rahul Sharngadhar. BSc. Optometry Mr. Mohan Nirmal MSc. Optometry, Mr. Nasser Al Shamali MSc. Optometry.
Case 1 presented to the emergency clinic 1-day after laser exposure complaining of poor vision in the left eye. On examination, the best corrected visual acuity was 6/6 with a refraction of −0.25 D sphere in the right eye and 1/60 with a refraction of −0.50–0.25 × 90° in the left eye with no improvement on pin-hole testing. Anterior segments and intraocular pressures were normal bilaterally Amsler grid testing was normal for the right eye and there was central scotoma in the left eye. On dilated fundus evaluation, the cup-to-disc ratios (CDR) were 0.4–0.5 bilaterally, the retinal vessels and fovea and fovea, in the right were normal. The left showed premacular subhyaloid hemorrhage approximately 1½ disc diameter [Figure 1]. Optical coherence tomography of the macula in the right eye was normal, in the left eye there was a shadow effect due to the subhyaloid haemorrhage [Figure 2]. The patient declined yittrium aluminium garnet (YAG) laser hyaloidotomy for the left eye. At 1-month follow up subhyaloid hemorrhage had completely resolved with a dull foveal reflex on fundus evaluation and no improvement in vision in the left eye [Figure 3]. Optical coherence tomography of macula in the left eye showed irregularity of the retinal layers [Figure 4]. Fluorescein angiography was un remarkable bilaterally [Figure 5].
(a) Fundus fluorescein angiography OD showing normal dye transit (b) fundus fluorescein angiography OS showing-normal dye transit
Articles from Middle East African Journal of Ophthalmology are provided here courtesy of Wolters Kluwer -- Medknow Publications
Multiple ocular symptoms such as pain, redness, irritation, corneal signs and retinal injury have been reported in patients exposed to laser pointers.1,2,3,4,5,6,7,8,9,10 Scotoma, photophobia, metamorphopsia, chromatopsia or decreased visual acuity can occur hours after exposure.1,2,3,4,5,6,7,8,9,10 The energy from the pointers at the ocular surface is insufficient to cause any appreciable harmful effect.4,5,6 However, amplification of irradiance caused by the ocular media to approximately 104 times makes the retina the most susceptible tissue in the body to laser pointer injury.7,8,9 Redness or surface irritation in a patient with laser pointer exposure is likely due to secondary rubbing of the eye. Pain following exposure to lasers may be due to corneal injury caused by eye rubbing following exposure.1,2,3,4,5
Circular polarizer linearvslinear
Retinal lesions following laser injury generally heal on their own, without any specific therapy. Systemic corticosteroids have been used, with little conclusive evidence indicating faster recovery.8,9,10 Hossein et al.9 noted clinical and objective improvement of laser induced maculopathy on spectral-domain optical coherence tomography in a patient who was treated with high dose systemic steroids. The patient was exposed to a class 3R laser for <1 s. Spectral domain optical coherence tomography disclosed a hyper-reflective band in the foveal region. After 1-week of treatment, the hyper-reflectivity resolved. However, residual disruption of the outer retinal layer at the fovea remained unchanged.9
Kasaoka et al.10 used animal models and reported that the RPE cells initiate a post-injury process in response to pathologic states and transform from a stationary epithelial state to a spindle-shaped, migratory, proliferative mesenchymal state, leading to the transretinal membrane formation associated with the development of proliferative vitreoretinopathy.10 This RPE transdifferentiation and its migration across the retinal surfaces is mediated by a tyrosinase receptor called c-Met. Control of this activity may be a future therapeutic target to minimize retinal damage following laser injury.9,10
Case 2 presented a week after laser exposure complaining of poor vision in the right eye. Best corrected visual acuity was 1/60 with a refraction of plano −0.25 × 85 in the right eye with no improvement with pinhole and 6/5 with a refraction of −0.50 −0.25 × 60° in the left eye. Anterior segment evaluation and applanation tonometry was normal bilaterally. Amsler grid testing indicated a central scotoma in the right eye and the left eye was normal. There was premacular subhyaloid hemorrhage in the right eye approximately 1 disc diameter in size covering the foveal area horizontally [Figure 6]. The retina in the left eye was unremarkable. Optical coherence tomography indicated a shadow effect due to the subhyaloid hemorrhage in the right eye and the left eye was unremarkable [Figure 7]. Fundus fluorescein angiograms indicated blocked fluorescence corresponding to the hemorrhage at the fovea in the right eye and was unremarkable in the left eye [Figure 8]. Hyaloidotomy with YAG laser was unsuccessful in the right eye as the blood covering the fovea was organised [Figure 6c]. The patient was subsequently lost to follow up.
Retinal injuries due to military and industrial lasers occur in less than 15 individuals yearly, world wide, despite the increasing use of lasers in the health care, military, and educational sectors, and in commercial laboratories.1 In the military, lasers are used as range finders, target designators and for long distance communications.1,2,3,4,5,6 Even in ophthalmology the use of lasers has increased significantly. The increase in the use of laser devices has resulted in a concomitant increase in ocular exposure to laser radiation. Accidental momentary laser exposure can be annoying and distracting.7,8,9,10 Prolonged viewing of the beam for more than 10 s especially at close range, can cause retinal damage.10
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
Very clear and excellent article, CJ. I had always wondered about that. You are spot on in your description about buying kits with such filters floating in the bag and the cheapo 2X int here as well haha. so true. Last Winter I enjoyed pulling al my filters out and giving them a good clean and cataloging. Only thing I would suggest differently is to buy correct size for all your lenses so you can maintain a hood on the lens, as POL is all about reduced glare anyway. That is where OM was such a brilliant system with a large number of lenses conveniently taking 49mm filters. And like you say, but good ones and they will survive most camera brand changes as you wisely grow into better quality kit as you get older.
Lasers are divided into four “classes” based on their output (Class 1 and 1 M, Class 2 and 2 M, Class 3A, 3B, 3R and Class 4).1,2,3 Class 1 lasers, (energy <0.4 mW) are the safest and cannot cause damage even if viewed for long periods of time. Class1 lasers are used in intrabeam viewing in optical instruments. Visible laser pointers (400–700 nm) operating at <1 mW and 1–5 mW power are Class 2 and Class 3A lasers respectively. Class 3B and 3R lasers generate between 5 and 500 mW of power; Class 4 lasers generate more than 500 mW of power.
Circular polarizer linearvspolarizer
(a) Optical CoherenceTomoraphy OD - macula normal (b) optical coherence tomoraphy OS showing fill thickness hole, cystoid changes at the edges, with increase reflectivity at the base of the hole
Linearpolarization
Anterior segment injuries are rare as the cornea and crystalline lens absorbs most of the UV and infrared energies. Natural responses such as the blink response, squinting, pupillary constriction, and aversion from the uncomfortably bright light protects the retina from accidental injury.1,2,3 Most often, retinal injuries are subtle with no objective findings making diagnosis of laser induced damage difficult. In such cases diagnosis is facilitated by a set of six questions formulated by Mainster et al.1 Visual prognosis is excellent if retinal findings are minor or spare the fovea.1,2,3,4,5,6

(a) Fundus fluorescein angiography OD - showing blocked fluorescence due to subhyaloid hemorrhage at posterior pole. (b) Fundus fluorescein angiography OS - normal dye transit
(a) Fundus photograph OD - premacular subhyaloid haemorrhage. (b) Fundus photograph OS normal. (c) Fundus photo graph OD - organised blood clot at posterior pole following yittrium aluminium garnet lysis
June 2024 April 2024 March 2024 February 2024 January 2024 June 2023 March 2023 December 2022 November 2022 October 2022 September 2022 August 2022 July 2022 June 2022 May 2022 February 2022 December 2021 October 2021 September 2021 August 2021 July 2021 June 2021 May 2021 April 2021 February 2021 January 2021 December 2020 November 2020 July 2020 April 2020 October 2019 August 2019 June 2019 May 2019 April 2019 March 2019 February 2019 December 2018 November 2018 October 2018 September 2018 August 2018 July 2018 June 2018 May 2018 April 2018 March 2018 February 2018 December 2017 September 2017 August 2017 July 2017 June 2017 April 2017 March 2017 February 2017 January 2017 November 2016 October 2016 September 2016 July 2016 June 2016 May 2016 April 2016 March 2016
Keywords: Fundus Fluorescein Angiography, Laser Pointer, Macular Hole, Optical Coherence Tomography, Subhyaloid Hemorrhage
Laser pointers are simple, handheld battery operated devices, used for teaching and training purposes. Laser pointers are comprised of a diode emitting laser light, with an energy output between 1 and 5 mW.1,2,3,4,5 Initially commercially available laser pointers were red lasers with a wavelength of 670 nm. However, other wavelengths such as green, blue, yellow and violet lasers are also available and have become popular because of their advantages. For example, green lasers have brighter beams visible both in daylight and night, allowing star gazing and pointing far off objects, blue and violet lasers light up to different colors depending upon where they are projected, yellow lasers dazzle like gold and are used as a laser guide star for use with astronomical adaptive optics.1,2,3,4,5,6,7 As the use of laser pointers becomes more popular, physicians need to understand which lasers can cause eye injury.1,2,3,4,5,6,7,8
Thanks for the thoughtful comment, Peter. Although I understand that current lens design generally prioritizes maximizing optical performance over the convenience of fewer filter sizes, I too can appreciate the '70s ethos of standardized filter sizes (Canon & Minolta @ 55mm, Nikon @ 52mm, and Olympus & Pentax @ 49mm) and then having two or maybe three more sizes at most to cover the rest of the lineup. It made things so much simpler in the accessories department for the photographer :-). Nikon today is a complete mess with 10 (count 'em) filter sizes with no standardization whatsoever. Best regards.
Transmission and absorption of optical radiation by ocular media depends upon the wavelength of the incident ultraviolet (UV) radiation, visible light or infrared radiation.5,6 For lasers, wavelength, spot size, pulse duration and irradiance determine the magnitude and extent of thermal damage in tissues exposed to the laser beam. Laser pointers emit invisible infrared radiation combined with visible light. Potential harmful effects to the eye, occur due to photomechanical, thermal or chemical injuries, or a combination of these effects.3,4,5,6,7 These effects are applied in a controlled manner for the treatment of eye diseases.1,2,3,4,5
All Buyer's Guide Camera Comparison Camera Profiles Canon Contax/Yashica Film Filters Flash Fuji History Kodak Konica Leica Lenses Mamiya Minolta Nikon Olympus Pentax Point & Shoots Rangefinders SLRs Tips Topcon



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500