
Microscope Objectives – magnification, focal length ... - what is the objective lens of a microscope
Laser cavitytypes
In a direct hernia, the peritoneal sac enters the inguinal canal directly via a defect or weakness in the posterior wall of the inguinal canal, usually the transversus abdominis. It usually protrudes directly to the abdominal wall but may exit through the external inguinal ring.
Cavitymodes inlaser
There are two known nerves that pass within the structures of the inguinal canal. These nerves are the ilioinguinal and the genitofemoral nerves. [1] A third nerve, iliohypogastric nerve, supply sensation to the skin above the genitalia does not pass through the inguinal canal. It pierces the transversus abdominis then the external oblique in the inguinal area.
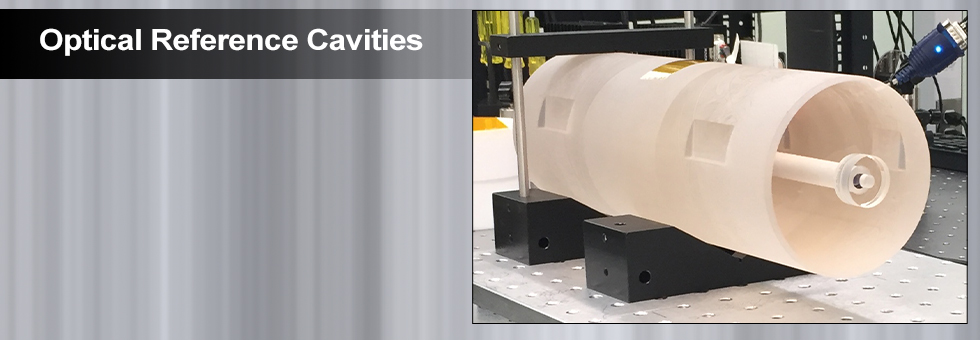
Optical reference cavities are resonators for light and provide a way to precisely define an optical frequency. Optical reference cavities are used analogously to tuning forks for musical instruments, which define a reference acoustic frequency; the ability to define an extremely precise optical “note” is a fundamental need in precision metrology. Whether implemented for the measurement of length displacements at the 10-18-meter level, which can be induced by transiting gravitational waves at facilities such as LIGO, Virgo, or KAGRA; the production of optical frequencies to a precision better than a single hertz for atomic clocks; or the detection of trace gases; optical reference cavities have become ubiquitous and indispensable tools for high-precision laser-based metrology and sensing.
At Thorlabs Crystalline Solutions, we offer a range of standard and custom crystalline mirrors for the near- and mid-infrared spectral regions that exhibit ideal properties for use as end mirrors in optical reference cavities. These “semiconductor supermirrors” (Figure 2 (left)) exhibit ultralow optical losses (including both scatter and absorption) and minimal Brownian noise, making them ideal for optical reference cavities for optical atomic clocks, high-finesse enhancement or ringdown cavities, and general, cavity-stabilized laser or comb systems. The high-quality-factor single-crystal coatings used in our xtal stable™ optics substantially reduce inherent thermomechanical fluctuations, enabling significant improvements over sputtered dielectric coatings in the overall frequency stability of precision interferometers. In this way, our crystalline mirror technology enables a reduction in the size of optical reference cavities, while simultaneously maintaining a low noise floor. For an in-depth investigation of thermal noise effects in optical metrology, we highly recommend the textbook edited by G. Harry, T. Bodiya, and R. DeSalvo, Optical Coatings and Thermal Noise in Precision Measurement from Cambridge University Press [4].
Laser cavitylength formula
We partnered with Wolfram® to create a web application that allows you to directly compare the optical cavity noise performance between our crystalline supermirror coatings and conventional ion-beam sputtered (IBS) coatings for a variety of cavity design parameters. The application may be accessed by clicking the link below:
Laser cavityalignment
The ilioinguinal nerve is a branch of L1. It passes through the deep inguinal orifice along with the cord structures. It provides sensation to the anterior perineum and medial and upper thigh. In males, it also provides sensation to the anterior scrotal area. In women, the nerve provides sensation to the labia majora and mons pubis.
Front of abdomen, showing surface markings for arteries and inguinal canal Henry Vandyke Carter, Public Domain, via Wikimedia Commons
The ilioinguinal and genital branch of the genitofemoral nerve pass with the cord structures close to the blood vessels course. Entrapment or injury is more likely to happen when wrapping the cord with the mesh or when dissecting the hernial sac. Iliohypogastric injury or entrapment is more likely to happen when suturing the mesh to the internal oblique/conjoint tendon or when closing the external oblique aponeurosis. The incidence of nerve injury after hernia repair is low but variable.[7]
The .gov means it's official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you're on a federal government site.
Minimally invasive hernia repair approach has been used increasingly in the last decade. Both the Totally Extra-Peritoneal (TEP) and Trans-Abdominal Preperitoneal (TAP) Approaches have been used. Minimally invasive repair involves less interruption of the inguinal canal structures. It includes reducing the hernial content and sac then re-inforcing the posterior inguinal wall pre-peritoneally by placing flat mesh centered on the hernia defect.
Typical ring-down signals and the residuals generated from a least-squares fit to the model y=ae(-t/τ)+b are shown in Figure 9. Additionally, the average of 50 consecutive ring-downs and their fit residuals are displayed, and there are no signs of non-exponential behavior at our highest levels of signal-to-noise ratio.
by NI Zheludev · 2008 · Cited by 253 — What diffraction limit? ... Several approaches are capable of beating the classical 'diffraction limit'. In the optical domain, not only are superlenses a ...
Laser cavityuses
Inguinal hernias are a common surgical disease. Understanding the anatomy of the inguinal canal is crucial for the identification and surgically repairing inguinal hernias. Surgical repair of inguinal hernias is based on repairing the hernial defect and reinforcing the posterior inguinal wall after reducing the hernial content and sac. Different methods of repair have been used in the past decades. Formerly, the repair was done by primarily closing the defect or approximating the edges of the widened inguinal ring to provide strength. It was noticed that the recurrence rate of this type of repair was unacceptably high. The explanation to this high recurrence is that the approximated tissue were put under high tension. Forcing the tissue to approximate will result in high tension on the defect edges. Over time, this tension will pull through the tissue resulting in the recurrence of the weakness and hernial defect. Therefore, It was realized that another material is needed to strengthen the posterior wall of the inguinal canal. The idea of using a mesh was then adopted. The mesh provides the necessary strength without exposing tissue to tension.
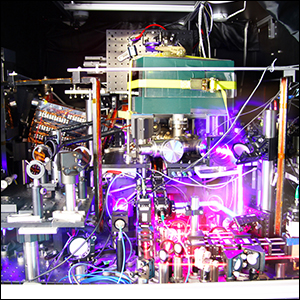
Figure 1: (Left) Photograph of a strontium optical clock constructed by researchers at the University of Colorado and the National Institute of Standards and Technology [2]. (Right) Aerial view of the Virgo gravitational wave observatory [3].
Sep 16, 2024 — What is DLC coating? Diamond-like carbon (DLC) coatings are nanocomposite layers that mimic the properties of natural diamond, offering low ...
When an individual develops increased intraabdominal pressure, the contents of the abdominal cavity push down on the inguinal ligament. To prevent herniation of the abdominal contents inside the inguinal canal, the posterior wall of the canal contracts while the muscles of the anterior wall tighten to narrow the canal.[8]
With a measured value of τ and the known cavity length, L, the total optical loss (T + S + A) of each supermirror is given by T + S + A = L / (cτ), where c is the speed of light. From the conservation of energy, the total loss and reflectivity are connected by 1 - R = T + S + A.
Coating optical loss mechanisms consist of transmission (T), scatter (S), and absorption (A), as shown in Figure 3. Collectively, scatter and absorption are known as excess optical losses, and are critical parameters for supermirrors. While transmission is typically a design parameter controlled by the layer structure of interference coatings, excess losses are generally harder to control beyond a minimum level driven by manufacturing and material imperfections. In the case of an optical cavity, the partition of losses between transmission and excess loss determines the usability of the cavity – if excess loss dominates, there is little difference between the on- and off-resonance levels of transmission, leading to poor optical frequency discrimination and poor signal-to-noise. Assuming perfect spatial mode matching of the input beam to the cavity, the fractional amount of power transmitted through the cavity is given by Pt /Pi = T2/(T+S+A)2, where Pt and Pi are the optical powers transmitted and incident on the cavity, respectively.
To address optical frequency sensitivity of such a compact reference cavity, we manufacture mirrors with a target and measured T of ~4 ppm. These mirrors are mapped to verify sufficiently uniform optical performance, with excess losses below 3 ppm, yielding a finesse in excess of 400 000 at 1397 nm in vacuum at room temperature. The inferred cavity transmission in this case is then close to Pt / Pi = 33%, assuming perfect spatial mode matching, and the inferred cavity full-width-at-half-maximum linewidth is 7.5 kHz.
In 1984, Anderson, et al. [6] described a reflectometer based on a resonant optical cavity comprising high-reflectivity end mirrors in order to convert an amplitude measurement into a pure time-delay measurement by exploiting the finite speed of light. When a pulse of incident light reaches the output mirror, a fraction equal to the transmission T is outcoupled and a fraction R is reflected back into the cavity (see Figure 6). On the second round-trip, the same fraction T of this now-reduced incident power is again out-coupled. This ratiometric progression of loss per round trip of the cavity leads to an exponential decay of the transmitted optical power with time constant τ. Critically, this technique is impervious to source amplitude fluctuations, and less sensitive to detector linearity, detection noise, and dynamic range limitations compared to other measurement techniques.
Precise and accurate determination of the quantities T and S + A presents a difficult measurement challenge due to the small values (typically 10 < T < 5 ppm and S + A < 5 ppm for our crystalline coatings) and dynamic range involved. For example, commercial spectrophotometry systems are relatively widely accessible, but will typically provide accuracies at a 0.3% (3000 ppm) level up to reflectivities of approximately 99.9%. Similarly, ratiometric laser power measurements providing 0.01% (100 ppm) accuracies for reflectivities up to 99.99% fall short for characterization needs of these supermirrors. Technical challenges include source amplitude stability, detector linearity over large ranges of optical inputs, and detection noise.
Optical reference cavities, in their simplest form, consist of two parallel low-loss, highly reflecting mirrors facing each other [1]. Resonant enhancement of the optical field inside the optical reference cavity is observed when the cavity length, L, is an integer multiple of λ/2, where λ is the wavelength of the light incident on the reference cavity. At resonance, a maximum amount of light is transmitted (instead of reflected, as occurs when the incident light is not on resonance), and the intracavity field is strongest. These properties of the optical cavity are exploited in different ways to achieve the remarkable measurement capabilities mentioned above.
The spermatic cord is easily recognized as it runs in the inguinal canal. It runs together with several small vessels and nerves that connect with the testis. The structures that are of importance in the spermatic cord include the testicular artery, artery to the vas deferens and the cremaster artery. In addition, there are lymphatics and the pampiniform plexus and the genital branch running with the cord. Any combination of these structures can be injured if the spermatic cord is handled inappropriately during surgical dissection.
The hernial sac protrudes through the femoral ring, the medial part of the femoral canal. Surgical repair of the femoral hernia is slightly different than inguinal hernias in the open approach. While it is the same in the minimally invasive approach.]
Zaber's RSB motorized rotation stages have a 120 mm table diameter and a 50.8 mm (2 inch) aperture. They feature a compact footprint, low profile, ...
A hydrocele occurs because of the persistent patency of the processus vaginalis, and it may coexist with an indirect hernia. The condition presents with fluid accumulation in the scrotum. The fluid accumulation can be significant, and most hydroceles need surgical intervention.

by SM Beck · 2005 · Cited by 386 — We investigate a technique known as synthetic-aperture imaging laser radar (SAIL), which employs aperture synthesis with coherent laser radar to overcome the ...
The total optical loss of every supermirror we ship is measured using a custom-built cavity ring-down system [7]. Figure 8 shows a simplified operational diagram of this setup. Diode lasers are directly coupled—without optical isolation—into a linear cavity formed from a pair of crystalline supermirrors. This arrangement greatly simplifies the system by removing the need for active laser stabilization. The retroreflection of the cavity input coupler forms an extended cavity diode laser and narrows the laser linewidth (as shown in the inset graph in Figure 8). The narrowed linewidth increases the in-coupled optical power by pulling the laser close to the center wavelength of the coating, where the composite laser and external cavity typically has the lowest loss. Irises ensure that the sampled points fall within a radius of 1.5 mm of the center of the mirror substrate. An InGaAs camera (owing to the infrared nature of our mirrors) is used to align the supermirrors and excite the fundamental TEM00 mode. A fast InGaAs photodiode detects the transmitted optical power and a digital delay generator [8] modulates the laser diode current to zero when the transmitted power exceeds a threshold voltage and triggers data acquisition of a single ring-down transient.
The anatomy of the inguinal canal is of paramount importance for the surgical management of inguinal hernias. As a natural canal with orifices, widening can develop to let other structures from the abdominal cavity pass through to the extra-abdominal space. Chronic increase in abdominal pressure is known to be the main cause of this type of hernias. Inguinal hernias are a common surgical problem that often necessitates surgical repair. A clear understanding of the anatomy of the area is crucial to do a proper surgical repair of the inguinal hernias.[3]
The inguinal area and canal are known with inguinal hernias. Inguinal and femoral hernias are collectively called groin hernias. Other surgical diseases like hydrocele, varicocele and undescended testis are encountered in the area but are less common.
Both inguinal hernias often present in the labia majora or inguinal area as swellings which are more prominent when the individual is upright.
With the descent of the testicles, a peritoneal outpouching called the processus vaginalis follows the testicles to the scrotum. Following the descent of the testicles into the scrotum, the processus vaginalis degenerates. This process of degeneration or obliteration may be delayed, or it may fail completely. Failure of closure of the pocessus vaginalis leads to the propensity to develop a number of abnormalities. Peritoneal fluid can travel down a patent processus vaginalis leading to the formation of a hydrocele. Persistent processus vaginalis may increase the risk of development of inguinal hernias.
Supermirrors are indispensable for modern optical metrology and find use in increasingly high-performance optical cavities from the cm to km length scales. Improvements in coating technology are now pushing the ultimate limits of optical performance, with T + S + A at the <5 ppm level, enabling finesse values well in excess of 500 000. At the same time, the use of ultrahigh purity and low-mechanical-loss monocrystalline-semiconductor-based interference coatings are enabling order-of-magnitude reductions in elastic losses. The ability to fabricate mirrors with simultaneously excellent optical and mechanical properties through the use of crystalline coatings has led to substantial progress beyond fundamental limitations in the length stability of cutting-edge optical resonators.
The assembly of the completed cavity ends with the contacting of ULE compensation rings to the back side of the mirrors. In terms of the theoretical noise performance, this cavity (including contributions from the ULE spacer, fused silica substrates, and crystalline coatings) has a Brownian-limited frequency noise PSD of 3.6 × 10-3 Hz2/Hz (at 1 Hz) corresponding to an Allan deviation flicker floor of 3.3×10-16 at 1 s of averaging. In this implementation, the fraction of the Brownian thermal noise contributed by the spacer, substrate, and coating is 5.5%, 64.5%, and 30% respectively. In contrast, a comparable cavity with IBS coatings and having the same optical quality would yield a Brownian-limited frequency noise PSD of 2.5×10-2 Hz2/Hz (at 1 Hz) corresponding to an Allan deviation flicker floor of 8.7×10-16 at 1 s of averaging. With amorphous mirrors, the fraction of the Brownian thermal noise due to the spacer, substrate, and coating is 0.8%, 9.4%, and 89.8% respectively. As can clearly be seen, the dielectric coatings are the key noise source in such a high-performance reference cavity and our semiconductor supermirrors can significantly reduce the limiting thermal noise.
The genitofemoral nerve is derived from the L1-L2 spinal nerve roots. It divided above the inguinal canal to the genital branch that passes through the deep inguinal ring with the cord structures, and the femoral branch that passes below the inguinal canal. It provides a motor function to the cremasteric muscle and sensory innervation to the scrotum (genital branch) and the upper thigh (femoral branch) in males, and labia in females.
In the development of our semiconductor supermirror technology, we have focused on the production of crystalline mirrors with ever increasing reflectance. This has been achieved through continuous improvements in our epitaxial growth and substrate-transfer coating processes, enabling the minimization of excess optical losses. To progress in these efforts, we have overcome challenges related to the verification of the optical properties of this new class of low-optical-loss elements, with a key advancement being the development and demonstration of a novel spatial scanning ringdown system. Our in-house characterization capabilities are unmatched and allow us to confidently deliver mirrors that meet our customers’ stringent requirements. Ultimately, these mirrors, when built into a cavity and incorporated in purpose-built metrological systems, are advancing the state-of-the art in timekeeping and spatial measurement processes, impacting fields such as quantum optics, the study of quantum many body systems, ultrasensitive trace gas detection, and ultimately cosmology and astrophysics via the development of low-loss and low-noise reflective test masses for next-generation gravitational wave detectors.
The inguinal canal is made of a floor, anterior wall, posterior wall, and a roof. The floor of the canal that is made of the inguinal ligament. The inguinal ligament is a thickened inferior portion of the external oblique aponeurosis. The anterior wall is made of the external oblique aponeurosis. The posterior wall is made of the transversalis muscle. The more complex part - the roof - is made of the combined fibers of the internal oblique and transversus abdominis muscle and aponeurosis including the conjoint tendon. The conjoint tendon constitutes the main part of the medial portion of the posterior wall. Understanding the inguinal anatomy well is essential to understand the various hernias in the region and to perform the different types of surgical repair. It is important for surgeons to note that the mid-inguinal point marks the area between the anterior superior iliac spine and the pubic symphysis. Deep in this location, the femoral artery in the pelvic cavity enters the lower limb. The femoral artery can only be palpated below the inguinal ligament.[4][5][6]
In addition to the production of high-performance and low-noise optical reference cavity end mirrors, we also offer optical reference cavity assembly services, employing optical contacting to rigidly mount a pair of mirrors to a given spacer. Customers can supply their own spacer and ultralow expansion (ULE) glass compensation rings or, alternatively, provide their desired specifications and work with our expert staff to design and manufacture a custom spacer. Thorlabs Crystalline Solutions will optically contact our crystalline coating mirrors to these components in an ISO class 1000 cleanroom facility. Adhesive-free direct bonding minimizes the number of contributors to Brownian noise to only the optical cavity's mirror coatings, mirror substrates, and spacers, increasing stability and measurement sensitivity. Following the assembly process, we can qualify the optical performance of the reference cavity before shipment. The details of our optical ringdown measurement scheme are presented in detail below.
Aug 2, 2018 — Seeing lens distortion in photography. Before you can purposefully use lens distortion or compression, you need to be able to notice it. I ...
An indirect hernia can occur when the peritoneal sac enters the inguinal canal via the deep inguinal ring. The hernia protrudes through the external inguinal ring. There is typically associated failure of the processus vaginalis atrophy after birth.
The 144-cell XXL solar modules are the best choice for ground-mounted systems where high performance counts. ○ 15 years manufacturer's warranty. ○ Highest ...
Optical reference cavities intended for use outside the laboratory in mobile experiments, or those onboard satellites in space, need to be compact in size due to payload limits. However, shorter reference cavities suffer two disadvantages. First, the sensitivity of optical frequency discrimination will decrease because the cavity linewidth increases for given mirror reflectivities. Second, the coating thermal noise becomes a greater contributor to the noise budget for decreasing cavity length.
Optical resonator inlaserpdf
After passing coating qualification, the mirrors are assembled into an optical cavity by contacting them to a 5-cm-long ultralow-expansion (ULE) glass spacer. The assembled cavity finesse is measured once again to confirm that the fully assembled cavity meets specifications and no dust or other fouling has degraded the mirrors during assembly. Should a cavity not meet specifications, the combined in-house mirror fabrication, cavity assembly and ringdown measurement capabilities allows rapid repair/replacement iterations as needed.
During embryogenesis, testicles descend from the posterior abdominal wall and gradually migrate into the scrotal area. This descent or migration movement of the testicles is guided by a cord-like structure called the gubernaculum. It attaches the inferior pole of the testicles to the developing scrotal sac.
Get Reflex Advanced Materials Corp (RFLXF:OTCQB) real-time stock quotes, news, price and financial information from CNBC.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
Critically, the optical cavity transmission rapidly drops to zero when the excess losses are much greater than T (Figure 4). For a given lowest workable value of cavity transmission Pt , the lowest achievable levels of excess loss will dictate the lowest practical value of T, which in turn determines the highest achievable finesse. Therefore, high-quality supermirrors need to be superb both in their low designed transmission value and as-deposited transmission value and in their ability to achieve low excess loss.
Laserresonator Pdf
The eyepiece (or ocular) is designed to project either a real or virtual image, depending upon the relationship between the intermediate image plane and the ...
Find the science equipment and materials needed to complete the lab content in your AOP Christian Homeschool curriculum with these lab kits from Home ...
Surgical repair of inguinal hernias is one of the most common general surgery procedure performed in the U.S. Open inguinal hernia repair includes opening the inguinal canal by incising the external oblique aponeurosis. The inguinal contents are mobilized and dissected to identify, isolate and reduce the hernial sac. Repair and re-inforcement of the posterior wall of the inguinal canal are done with synthetic flat mesh sutured to the inguinal peri-tubercular tissue, incurved part of the inguinal canal, and the conjoint tendon tissue.
While the development of this scanning cavity ringdown apparatus was initially developed for internal process development, we can now offer coating loss mapping as a service for mirrors operating at 1064 nm, 1156 nm, 1397 nm, 1550 nm, and 1572 nm.
The inguinal area is also associated with lymph nodes drainage basin and consequently lymphadenopathy from infections and malignancies. Primary malignancies in the inguinal area are rare, but a lymphoma can present with bilateral lymphadenopathy of the groin. Secondary lymphadenopathy from primary malignancies in the lower limbs, like skin melanoma, are not uncommon. Lipoma of the spermatic cord and malignant tumors like rhabdomyosarcomas are other known tumors of the inguinal area.
By mounting the supermirrors on motorized mounts with four degrees of freedom (two angular and two translational), the optical loss from each coating (including curved mirrors) can be spatially mapped. Figure 10 shows an example of a discarded coating exhibiting a constellation of defect sites that was mapped in this way. Complete correlation of the high optical loss regions to visible coating defects was established by comparison to differential interference contrast microscopy. (See Reference [7] for a more complete discussion on the measurement technique and mapping system.)
During inguinal hernia surgery, great care is required to prevent damage to the nerves as it can lead to significant morbidity. In hernia repairs that utilize a mesh the ilioinguinal and genital nerves can be compressed while suturing around the internal oblique muscle. Postoperatively the patient will complain of significant pain or tingling in the innervated areas.
Laser cavityfilling
Failure of the testicles to descend may result in various degrees of undescended testes. This is a common pediatric surgical problem.
Even for identical optical losses (leading to identical finesse and cavity transmission), not all supermirrors are created equal! In applications where the reference cavity length noise arising from the thermal atomic motion in the coating matters (e.g. in the construction of narrow-linewidth lasers with active locking to an optical cavity, or precision displacement sensing as with gravitational wave detectors), the mechanical material properties also become important [4]. Monocrystalline semiconductor materials such as GaAs/AlGaAs exhibit quasi-bulk properties and lower mechanical noise than amorphous, dielectric coatings created from sputtering, as shown in Figure 5. The reduction in elastic losses in these materials, which is quantified by the mechanical loss angle, Φ, the imaginary component of a complex Young’s modulus E(f ) = E0[1+i Φ(f )], is a consequence of the nearly flawless crystal lattice created by molecular beam epitaxy. The resulting >10× reduction in Φ for our crystalline coatings results in a reduction of the frequency-dependent noise power spectral density (NPSD) by a factor of √Φ in a properly designed reference cavity, when compared to amorphous mirror coatings deposited with processes such as ion-beam sputtering [5].
Imaging Edge Desktop (Remote/Viewer/Edit) 2.1.00 (Mac) has been released. Added support for macOS 10.15. Added support for simple creation of Time-lapse movies ...
Commonly, the cavity finesse F = cπτ / L is also used to describe the optical loss of a reference cavity. For a simple linear optical cavity consisting of two mirrors, the finesse is related to the reflectivity of each mirror by F = π√R / (1 - R). Figure 7 shows that few-ppm levels of deviation in losses lead to large changes in finesse for high-finesse cavities (e.g., above 200 000), making control over these losses extremely important for these applications.
Inguinal Region. This image includes the inferior epigastric artery and vein, rectus abdominis muscle, internal inguinal ring, Hesselbach triangle, inguinal ligament, inguinal canal, external inguinal ring, femoral ring, femoral vein, femoral (more...)
The inguinal region is a relatively anatomically complex region. Amon the several clinically important structures, it contains the inguinal canal which will be the focus of this article. The inguinal canal is a passage in the lower anterior abdominal wall located just above the inguinal ligament. It starts from the internal inguinal orifice, extends medially and inferiorly through the abdominal wall layers and ends in the external inguinal orifice. This canal is about four to six centimeters in length. The length changes from over the growth period from the pediatric age to adulthood. It functions as a passageway for structures between the intra- and extra-abdominal structures. In males, it transmits the spermatic cord, gonadal vessels, and lymphatics. While in females, it transmits the round ligament of the uterus[1][2]. The clinical significance of the area comes from the common surgical problem of inguinal hernias, and to a lesser extent, the inguinal lymphadenopathy and varicocele.
This book is distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0) ( http://creativecommons.org/licenses/by-nc-nd/4.0/ ), which permits others to distribute the work, provided that the article is not altered or used commercially. You are not required to obtain permission to distribute this article, provided that you credit the author and journal.



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500