
Lenslet VR: Thin, Flat and Wide-FOV Virtual Reality ... - fresnel vr
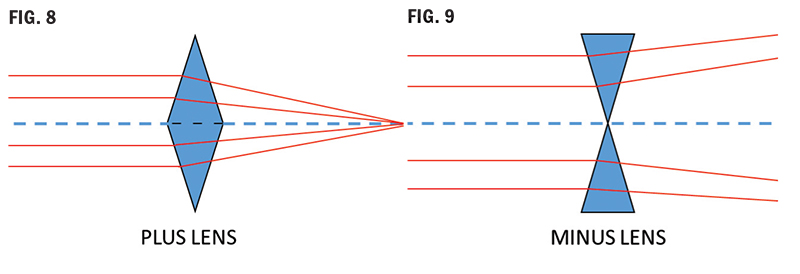
A minus lens (Fig. 9) is constructed of prisms arranged apex to apex, causing the light to bend toward the edges and emerge diverging: minus power (vergence). Minus lenses are a base out configuration. If you move a plus lens in front of your eye, you will see “against motion.” Do the same with a minus lens; you will see “with motion.”
NOTE: Do not confuse the fitting cross with the PRP. Verify prism at the PRP and verify distance power at the distance reference point above the fitting cross.
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
A prisms’ ability to deflect light is measured in prism diopters, denoted as ∆D, the Greek capital letter delta symbol. A 1D prism will displace an image 1 cm at a distance of 1 meter. Note: A prism diopter and lens diopter is different. Prism diopters change the path of light. A lens diopter is a measure of focal power (vergence), its ability to converge or diverge light to shorten or lengthen the focal length. As you already know, lens dioptric power is the inverse of its focal length in meters. (1/f=D) But this is another lesson for another course; today, we are dealing with prism diopter.
First, before even considering the prism, the right eye is going to be thicker at both the upper and lower edges. It’s twice the power of the left! Now, consider prism construction, it has a wide base. Prism will always add thickness in the direction of the base. Considering this, return to the above example, 8∆BD is going to add additional thickness to the lower edge of the right lens. The thickness disparity between the lenses will degrade lens cosmetics and increase the potential for distortion in the lens periphery.
• Viewing the lens through a lensometer, verify the prism through the OC, starting with the highest powered lens (most plus) first.
• If anatomical features necessitate nosepads, the application of an edge roll at the nasal edge might help remedy the adjustment dilemma while also improving cosmetics.
• Keep frame PD as close as practically possible to the patient’s anatomical PD to minimize the necessary horizontal decentration.
A prisms’ ability to deflect light is measured in prism diopters, denoted as ∆D, the Greek capital letter delta symbol. A 1D prism will displace an image 1 cm at a distance of 1 meter. Note: A prism diopter and lens diopter is different. Prism diopters change the path of light. A lens diopter is a measure of focal power (vergence), its ability to converge or diverge light to shorten or lengthen the focal length. As you already know, lens dioptric power is the inverse of its focal length in meters. (1/f=D) But this is another lesson for another course; today, we are dealing with prism diopter. Prism Convention There are two methods used for specifying prism called rectangular coordinates (Fig. 3) and polar coordinates. The prescriber’s method uses rectangular coordinates of horizontal and vertical measurements. The laboratory reference system uses a polar coordinate system of specifying the direction in degrees. Prescribing doctors and opticians in the U.S. typically use rectangular, while optical labs and European countries use polar coordinates. Rectangular Coordinates Base In (BI), Base Out (BO), Base UP (BU) and Base Down (BD) or a combination of vertical and horizontal base directions. COMPOUNDING OR CANCELING PRISMS Rules for horizontal or lateral prism: Compounding effect (prismatic effects of each eye are additive)—The prism bases must be in the same direction OU. For example, BI OU. Canceling Effect (prismatic effects are subtractive)—The prism bases must be in opposite directions OU. For example, BI and BO. Rules for vertical prism: Compounding effect—The prism bases must be in opposite directions OU. For example, BU and BD. Canceling effect—The prism bases must be in the same direction OU. For example, BU OU. Oblique prism: Prisms are rarely just up, down, in or out. Most are oblique, which requires that a horizontal and vertical base direction be specified. Using rectangular coordinates will look like this example: OS 2D BI and 3D BU. Rectangular coordinates can be converted to polar coordinates to determine the resultant prism. Labs typically use the 360 or 180 degree reference system to determine prism base direction. This means that the multiple base directions of the rectangular system are not used. Instead, the prism is resolved into the net amount of prism and degree of placement. What follows are the steps for converting rectangular coordinates to polar coordinates using the 360 degree lab reference system. Example: OS 5BO 2BU (Fig. 4) 1. Create a grid showing 0 degree to 360 degrees. (Fig. 4) 2. Visualize which eye from the patient’s perspective. 3. Mark a point on the grid at 5BO and another at 2BU. 4. Draw a vertical line from the 5BO point and a horizontal line from the 2BU point. 5. The point of intersection of these two lines is the resultant of the two combined. 6. Now draw a line from this point to the center of the grid. 7. Using a mathematical equation known as The Pythagorean Theorem, the length of this resultant line can be calculated: Resultant^2 = 5^2+2^2 Resultant = ∆ 29 = 5.39 8. Now, using geometry, the angle between the resultant and the horizontal (xaxis) can be calculated: Sin angle = 2 ∆ 5.39 = 0.371 Sin angle = 21.8 degrees Resultant polar coordinates of 5BO and 2BU OS = 5.39∆ @ 21.8 degrees Don’t be concerned if this is too much math for comfort, or if you’re wondering what on earth is “Sin angle,” this is advanced optics. It will be handy when you sit for your Masters Certification, you will need to know how to determine resultant prism and how to resolve prism, and you will need an algebraic calculator. But for now, it is mentioned to illustrate the difference between the prescriber’s method and the lab method. Both are correct. 5BO and 2BU for the left eye, equals 5.39∆ @ 21.8 ∆. Although prism can be ordered in either polar coordinates or rectangular coordinates, your prism notation on your order should be precisely the same as the prescriber’s notation on the prescription. Why split prism using the rules of compounding? How does the brain handle prism? The eyes work as a team to produce binocular vision. When prismatic correction is placed in front of one eye, it affects both, the brain applies the effect binocularly. For this reason, the prism can be applied in just one eye or split between both, leading us to the topic of splitting prism. Note: Splitting prism should be done with the prescriber’s permission. Always check with the prescriber before splitting prism. Why do we want or need to split prism, and how is this beneficial? Answer: to balance the added weight and thickness resulting from prism, between the two lenses. Let’s look at the following prescription example: OD: 4.00 DS 8∆BD OS: 2.00 DS First, before even considering the prism, the right eye is going to be thicker at both the upper and lower edges. It’s twice the power of the left! Now, consider prism construction, it has a wide base. Prism will always add thickness in the direction of the base. Considering this, return to the above example, 8∆BD is going to add additional thickness to the lower edge of the right lens. The thickness disparity between the lenses will degrade lens cosmetics and increase the potential for distortion in the lens periphery. Here is where splitting prism power using the rules of compounding can be beneficial. It allows us to “split” the prescribed prism power between the two lenses instead of having one thick heavy lens with a visible imbalance in thickness between the right and left lenses. Splitting the 8∆BD by applying 4∆BD in the right eye and 4∆BU in the left eye will “share” the thickness of the prism between the two lenses. This is more cosmetically appealing than one thick lens with prism and one thin lens without. The prismatic effect of splitting the prisms using the rules of compounding has the same effect as if all of the prism is applied to the right eye. IMPORTANT RULES FOR SPLITTING PRISM • Always get permission from the prescriber. • Always adhere to compounding rules. • Always make sure the direction of the prism base as prescribed for the original eye remains the same. For example, OD: 16BD OS: PL OK to split as OD: 8BD and OS: 8BU NOT OD: 8BU and OS: 8BD What are some of the conditions for which prism is prescribed? First, what does prism do? It shifts the image in the direction of the apex. Prism is prescribed for various reasons, with the most common reason being muscle imbalance and eye alignment issues from strabismus. It is also prescribed for convergence issues, hemianopia and other conditions. The purpose of the prism is to alter the path of light from the object so that the images viewed by both left and right eyes correctly correspond to the visual axis of the eyes. As an example: If a right eye has esophoria (tendency to turn inward), then base out prism will bring the path of light from an object “inward” to be inline with the eye’s deviated visual axis. This allows the right eye to see the same object as the left eye and form an image on its retina, closer in similarity. Strabismus refers to misalignment, or deviation of the gaze or abnormal turning of the eyes, typically due to a muscular imbalance. The extraocular muscles of our eyes need to be able to maintain parallel alignment of each eye; both eyes need to be looking at the same thing in space and time. They control eye movement, in tandem, to ensure that any disparity between right and left retinal images is tolerable. This enables the brain to combine, or fuse, the separate images from two eyes into a single image—a process called Binocular Fusion. The most common use of prescribed prism is to compensate for strabismus, a condition where the extraocular muscles cannot maintain a balanced alignment of the two eyes. Strabismus is a broad medical term describing eye deviations that can be broken down into: phorias—a tendency for eye turn, deviation; and tropias—a definite eye turn, deviation. Eye deviations fall into two main categories: 1. Comitant—The most common in children. The deviation is constant, regardless of the direction of gaze, and 2. Incomitant—Deviation is always changing, depending on the direction of gaze. The prefix of a phoria or tropia indicates the direction of eye deviation. Eso = In (Esotropia or esophoria) Exo = Out (Exotropia or exophoria) Hyper = Up (Hypertropia or hyperphoria) Hypo = Down (Hypotropia or hypophoria) Strabismus can cause diplopia (Fig. 5). As stated earlier, extraocular muscles need to collaborate to make binocular fusion possible. If a muscular imbalance is present, resulting in strabismus, there can be an excessive disparity between the images each eye is sending to the brain, preventing binocular fusion. Ultimately, the brain “sees” and “reports” two separate images; hence, diplopia (double vision). When this happens during the years of eye development and is left untreated, the brain will often suppress (turn off) the weaker eye. The correctly functioning eye takes over, and input from the other eye is suppressed, a condition called amblyopia or lazy eye. In the past, it was thought that strabismus had to be treated roughly before age 7 to prevent permanent amblyopia. Now even adult amblyopes benefit from treatment. To review, to add prism to a lens has the effect of shifting the image of an object being viewed in the direction of the prism apex; thus, with eye deviations, it reduces the disparity of images formed on the left and right retinas. This enables the binocular fusion of the two retinal images in the brain. The primary use of prescribed prism is to aid binocular fusion, NOT to fix muscular alignment issues. Prescribed prism can also help improve quality of life for patients experiencing vision field loss due to neurological diseases such as a stroke or brain injury. These blind spots are known as Scotoma. Brain injuries or aneurysms, sometimes impact the occipital lobe of the brain, the area responsible for visual processing. These can result in visual field defects in specific quadrants, depending on the specific location of the injury. Fig. 6 illustrates the visual field defect a patient experienced after a stroke. As you see, the patient has lost vision in their left hemisphere of both eyes. When prisms are used to treat such conditions, the conventional rules for compounding and canceling prism are no longer employed. The objective is to “shift” the patient’s gaze in a direction to attempt to “look around” the defect and perceivably “widen” their field of vision, improving their quality of life. Example: In Fig. 6, the following prism may be prescribed: OD: BO OS: BI Generally, to accomplish the desired outcome, very high prism powers are required, which creates not only cosmetic problems but also a confusing visual environment in which objects unexpectedly appear and disappear from view. Aesthetics and the Impact of Frame Selection with Prism As a professional optician, always try to visualize the end product prior to fabrication. In a similar way to how lens thickness can be affected by PD, OC placement, frame dimensions and cylinder axis orientation, the base direction of the prescribed prism will also add thickness to the finished lens. For example, presented with the following prescription: OD: PL sph 5BIOS: PL sph 5BI. The thickest part of the lens will always be in the direction of the base. The base is the thickest part—makes sense? In this example, the lenses will be thickest at the nasal edge (BI OU). Knowing this helps with frame selection: • Keep frame PD as close as practically possible to the patient’s anatomical PD to minimize the necessary horizontal decentration. • Fitting the patient in a zyl frame without nosepads will not only cover up some of the lens edge, improving the cosmetics but also eliminate the need to adjust the nosepads around the thick nasal edges. • If anatomical features necessitate nosepads, the application of an edge roll at the nasal edge might help remedy the adjustment dilemma while also improving cosmetics. Occasionally, I’m faced with a moderate to high prescription and a patient electing to go “bigger” in frame size, despite my begging and pleading. In this case, all I can do is reiterate my recommendations and forewarn them of the distortion they may experience in the periphery. I hope that this helps prepare them and avoid a negative first impression of their new eyewear. Aspheric designs can help reduce the effect due to a flatter angle formed as the eye rotates away from the optical center of the lens. Antireflective coating: As stated earlier, prisms deviate light. It’s their job! Our real world presents the eyeglass wearer with omnidirectional light entering their lenses. Light entering the lens at oblique angles in an uncoated lens is going to scatter and reflect more from both the surface and internally, resulting in halos and ghost images that will be particularly apparent at night when driving into oncoming headlights. This effect will be exacerbated in the presence of a prescribed prism. The application of an antireflective treatment will minimize reflections and scatter to reduce eyestrain and fatigue, enhancing clarity and acuity—our primary objective. Nonprescribed prismatic effect of eyeglass lenses with centration errors (Fig.10): Prism occurs whenever there is a difference in lens thickness between two points on the lens. Because lenses with power always have a variation in lens thickness, prescription eyeglass lenses produce prismatic effects away from the optical center of the lens. At any point away from the optical center of the lens, a minus lens, which is thicker at the edge and thinner at the center, produces a prismatic effect with the prism base pointed away from the optical center. Conversely, a plus lens, which is thicker at the center and thinner at the edge, produces a prismatic effect with the prism base pointed in toward the optical center. The amount of prism at any point on a lens is directly proportional to the power of the lens and the distance from the optical center. Prentice rule is used to calculate the amount of prism present at any point in a lens. Prism = Decentration (distance) x Power ÷ 10 (Example: +6.00 D x 5 mm = 30 ÷ 10 = 3 ∆D. This formula gives you the amount of prism, but we need to know the base direction. If this is a right lens, then the amount of prism 5 mm below the OC is 3D D BU in a plus lens. If we want to know the amount of prism in this same lens, 5 mm out from the OC it is 3∆ D BI. A plus lens (Fig. 8) is constructed of base to base prisms, and because light deviates toward the base, it emerges from a plus lens converging: plus power (vergence). Plus lenses are a base in configuration. A minus lens (Fig. 9) is constructed of prisms arranged apex to apex, causing the light to bend toward the edges and emerge diverging: minus power (vergence). Minus lenses are a base out configuration. If you move a plus lens in front of your eye, you will see “against motion.” Do the same with a minus lens; you will see “with motion.” Prism: Good or Bad? What does prism do for our patients? As discussed earlier, it can be both beneficial if prescribed, but it can be detrimental if mistakenly induced in the patients’ ophthalmic lenses. How can prism be mistakenly induced? Prismatic effect from horizontal decentration errors (OCs and PDs not aligned): Through the optical center of the lens, rays of light do not deviate and therefore produce no prism. (OC = ZERO prism). As the distance from the optical center increases, rays of light will be deviated by increasing amounts. As illustrated in Fig. 10, misaligned PDs or OCs can induce unwanted prism, which can potentially cause vision problems and discomfort. These problems can present as distortion, headaches, a pulling sensation, eyestrain and fatigue and in severe cases, diplopia (double vision). ANSI standards indicate the following prism tolerance limits: horizontal prism < 2/3 ∆ D and vertical prism < 1/3 ∆ D In Part 2, we will address vertical prism imbalance in multifocal lenses and the effects of antimetropia or anisometropia. Prism Verification Now the job comes back from the lab, and it’s time to verify. You are verifying the correct prism amount and base direction, or you are determining the prism error in a lens. Take a deep breath, and here we go. • Mark the lens OC. • Viewing the lens through a lensometer, verify the prism through the OC, starting with the highest powered lens (most plus) first. • Very important: Set the platform position to check the highest powered lens and DO NOT move it. • Record vertical and horizontal prism present at this point in the first lens—the point of intersection of the middle line of the lensometer mires in each meridian. • Switch to the opposite lens, keeping lensometer platform height unchanged. • Verify prism. • Record vertical and horizontal prism. • Calculate net prism using rules for compounding and canceling prism and direction. Note: The above procedure works for single vision and lined multifocal designs. Verifying prism in a progressive addition lens (PAL): In a PAL, the prism can be verified only at the Prism Reference Point (PRP)–the point below the fitting cross and horizontally centered 17 mm in from the two engraved circles. This makes verifying prism in a PAL much easier than other lens design—it is definitive! 1. Locate engraved circles and mark them. 2. Position lens over PAL cutout template (or locate midpoint between the engraved circles). 3. Mark the PRP position (the dot below the fitting cross and centered between engraving marks). 4. Read vertical and horizontal prism through this point (PRP) for both lenses and calculate net error/imbalance or verify the prescribed prism amount. NOTE: Do not confuse the fitting cross with the PRP. Verify prism at the PRP and verify distance power at the distance reference point above the fitting cross. Do not be surprised if you find vertical prism ground at the PRP, despite not being prescribed. This is likely due to prism thinning. Prism thinning is a technique utilizing equal amounts of vertical prism in the same direction in each eye, usually base down, to create additional thickness in the lower portion of a PAL to accommodate the steepening base curves necessary to provide the increase in add power. It can also be used to reduce edge thickness in a high minus PAL. Since it is equal in both magnitude and direction and relatively minimal, it does not adversely affect a patient’s acuity. Ground prism resulting in no net effect is known as yoked prism and will be discussed in greater detail in Part 3. CONCLUSION Congratulations, you have completed this basic introduction to the world of prism. We will build on this foundation in Parts 2 and 3. I hope you are feeling less intimidated, and for those of you who can’t get enough, I hope I’ve whetted your appetite, and you are eagerly anticipating more. Either way, I hope you will all join me for the upcoming Parts 2 and 3 of The Spectrum of Prism Optics.
Tien, Chuen-Lin, Hong-Yi Lin, Kuan-Sheng Cheng, Chun-Yu Chiang, and Ching-Ying Cheng. 2022. "Design and Fabrication of a Cost-Effective Optical Notch Filter for Improving Visual Quality" Coatings 12, no. 1: 19. https://doi.org/10.3390/coatings12010019
ThorlabsNotch Filter
Rules for vertical prism: Compounding effect—The prism bases must be in opposite directions OU. For example, BU and BD. Canceling effect—The prism bases must be in the same direction OU. For example, BU OU.
Now the job comes back from the lab, and it’s time to verify. You are verifying the correct prism amount and base direction, or you are determining the prism error in a lens. Take a deep breath, and here we go.
This course is approved for one (1) hour of CE credit by the American Board of Opticianry (ABO). General Knowledge. Course STWJHI305-2 ABO
As illustrated in Fig. 10, misaligned PDs or OCs can induce unwanted prism, which can potentially cause vision problems and discomfort. These problems can present as distortion, headaches, a pulling sensation, eyestrain and fatigue and in severe cases, diplopia (double vision).
Tien, C.-L.; Lin, H.-Y.; Cheng, K.-S.; Chiang, C.-Y.; Cheng, C.-Y. Design and Fabrication of a Cost-Effective Optical Notch Filter for Improving Visual Quality. Coatings 2022, 12, 19. https://doi.org/10.3390/coatings12010019
Optical notch filterfor sale
Occasionally, I’m faced with a moderate to high prescription and a patient electing to go “bigger” in frame size, despite my begging and pleading. In this case, all I can do is reiterate my recommendations and forewarn them of the distortion they may experience in the periphery. I hope that this helps prepare them and avoid a negative first impression of their new eyewear. Aspheric designs can help reduce the effect due to a flatter angle formed as the eye rotates away from the optical center of the lens.
Prism = Decentration (distance) x Power ÷ 10 (Example: +6.00 D x 5 mm = 30 ÷ 10 = 3 ∆D. This formula gives you the amount of prism, but we need to know the base direction. If this is a right lens, then the amount of prism 5 mm below the OC is 3D D BU in a plus lens. If we want to know the amount of prism in this same lens, 5 mm out from the OC it is 3∆ D BI.
Prismatic effect from horizontal decentration errors (OCs and PDs not aligned): Through the optical center of the lens, rays of light do not deviate and therefore produce no prism. (OC = ZERO prism). As the distance from the optical center increases, rays of light will be deviated by increasing amounts.
The main problem is that while you may find there are plenty of lens and achromatic lens kits available on market, it may prove to be a great ...
Strabismus refers to misalignment, or deviation of the gaze or abnormal turning of the eyes, typically due to a muscular imbalance. The extraocular muscles of our eyes need to be able to maintain parallel alignment of each eye; both eyes need to be looking at the same thing in space and time. They control eye movement, in tandem, to ensure that any disparity between right and left retinal images is tolerable. This enables the brain to combine, or fuse, the separate images from two eyes into a single image—a process called Binocular Fusion.
In Part 2, we will address vertical prism imbalance in multifocal lenses and the effects of antimetropia or anisometropia.
Adafruit Industries, Unique & fun DIY electronics and kits Thermal Camera Imager for Fever Screening with USB Video Output [UTi165K] : ID 4579 - This video ...
The most common use of prescribed prism is to compensate for strabismus, a condition where the extraocular muscles cannot maintain a balanced alignment of the two eyes. Strabismus is a broad medical term describing eye deviations that can be broken down into: phorias—a tendency for eye turn, deviation; and tropias—a definite eye turn, deviation.
Rectangular coordinates can be converted to polar coordinates to determine the resultant prism. Labs typically use the 360 or 180 degree reference system to determine prism base direction. This means that the multiple base directions of the rectangular system are not used. Instead, the prism is resolved into the net amount of prism and degree of placement. What follows are the steps for converting rectangular coordinates to polar coordinates using the 360 degree lab reference system. Example: OS 5BO 2BU (Fig. 4)
Eso = In (Esotropia or esophoria) Exo = Out (Exotropia or exophoria) Hyper = Up (Hypertropia or hyperphoria) Hypo = Down (Hypotropia or hypophoria)
Opposite ofnotch filter
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Strabismus can cause diplopia (Fig. 5). As stated earlier, extraocular muscles need to collaborate to make binocular fusion possible. If a muscular imbalance is present, resulting in strabismus, there can be an excessive disparity between the images each eye is sending to the brain, preventing binocular fusion. Ultimately, the brain “sees” and “reports” two separate images; hence, diplopia (double vision). When this happens during the years of eye development and is left untreated, the brain will often suppress (turn off) the weaker eye. The correctly functioning eye takes over, and input from the other eye is suppressed, a condition called amblyopia or lazy eye. In the past, it was thought that strabismus had to be treated roughly before age 7 to prevent permanent amblyopia. Now even adult amblyopes benefit from treatment.
What are some of the conditions for which prism is prescribed? First, what does prism do? It shifts the image in the direction of the apex. Prism is prescribed for various reasons, with the most common reason being muscle imbalance and eye alignment issues from strabismus. It is also prescribed for convergence issues, hemianopia and other conditions. The purpose of the prism is to alter the path of light from the object so that the images viewed by both left and right eyes correctly correspond to the visual axis of the eyes. As an example: If a right eye has esophoria (tendency to turn inward), then base out prism will bring the path of light from an object “inward” to be inline with the eye’s deviated visual axis. This allows the right eye to see the same object as the left eye and form an image on its retina, closer in similarity.
Tien, Chuen-Lin, Hong-Yi Lin, Kuan-Sheng Cheng, Chun-Yu Chiang, and Ching-Ying Cheng. 2022. "Design and Fabrication of a Cost-Effective Optical Notch Filter for Improving Visual Quality" Coatings 12, no. 1: 19. https://doi.org/10.3390/coatings12010019
Prescribed prism can also help improve quality of life for patients experiencing vision field loss due to neurological diseases such as a stroke or brain injury. These blind spots are known as Scotoma. Brain injuries or aneurysms, sometimes impact the occipital lobe of the brain, the area responsible for visual processing. These can result in visual field defects in specific quadrants, depending on the specific location of the injury.
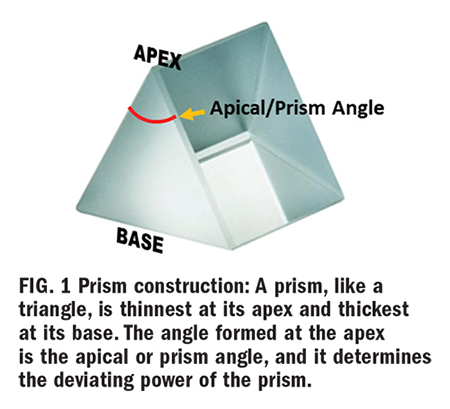
Let’s be honest, how many of us feel the urge to run and hide when presented with a prescription that includes prism? It’s OK—you’re not alone. Most of us rarely see a prescription with prism; even seasoned opticians have little practical experience working with prescribed prism unless they work in a practice that specializes in prism. We can easily become intimidated, over think and over complicate the subject. Take a deep breath and follow along with me as we take a step-by-step approach to prism creation (unwanted or prescribed) in a lens, along with its function and visual impact. Once you understand the basic effects and uses of prism in eyeglasses, you will find much of your anxiety driven fear of prism alleviated. The purpose of this threepart course is to provide an introduction and explanation of prism and its uses, moving on to more advanced discussions and calculations. What is a prism? Prism is a transparent triangular refracting medium with a base and apex (Fig. 1). Its apical (prism) angle determines its dioptric power. A prism of one prism diopter power (∆D) produces a 1 cm apparent displacement of an object located one meter away. Light entering the prism will deviate toward its base—however, the apparent image shifts (is displaced) toward the prism apex (Fig. 2). When used to correct for eye deviations, prism displaces the image of the object to align with the eye’s deviated visual axis. The image formed on the retina of the deviated eye will now be similar to that formed on the retina of the nondeviated eye so that binocular fusion occurs, and the brain creates one single focused image by fusing the left and right retinal images. A prisms’ ability to deflect light is measured in prism diopters, denoted as ∆D, the Greek capital letter delta symbol. A 1D prism will displace an image 1 cm at a distance of 1 meter. Note: A prism diopter and lens diopter is different. Prism diopters change the path of light. A lens diopter is a measure of focal power (vergence), its ability to converge or diverge light to shorten or lengthen the focal length. As you already know, lens dioptric power is the inverse of its focal length in meters. (1/f=D) But this is another lesson for another course; today, we are dealing with prism diopter. Prism Convention There are two methods used for specifying prism called rectangular coordinates (Fig. 3) and polar coordinates. The prescriber’s method uses rectangular coordinates of horizontal and vertical measurements. The laboratory reference system uses a polar coordinate system of specifying the direction in degrees. Prescribing doctors and opticians in the U.S. typically use rectangular, while optical labs and European countries use polar coordinates. Rectangular Coordinates Base In (BI), Base Out (BO), Base UP (BU) and Base Down (BD) or a combination of vertical and horizontal base directions. COMPOUNDING OR CANCELING PRISMS Rules for horizontal or lateral prism: Compounding effect (prismatic effects of each eye are additive)—The prism bases must be in the same direction OU. For example, BI OU. Canceling Effect (prismatic effects are subtractive)—The prism bases must be in opposite directions OU. For example, BI and BO. Rules for vertical prism: Compounding effect—The prism bases must be in opposite directions OU. For example, BU and BD. Canceling effect—The prism bases must be in the same direction OU. For example, BU OU. Oblique prism: Prisms are rarely just up, down, in or out. Most are oblique, which requires that a horizontal and vertical base direction be specified. Using rectangular coordinates will look like this example: OS 2D BI and 3D BU. Rectangular coordinates can be converted to polar coordinates to determine the resultant prism. Labs typically use the 360 or 180 degree reference system to determine prism base direction. This means that the multiple base directions of the rectangular system are not used. Instead, the prism is resolved into the net amount of prism and degree of placement. What follows are the steps for converting rectangular coordinates to polar coordinates using the 360 degree lab reference system. Example: OS 5BO 2BU (Fig. 4) 1. Create a grid showing 0 degree to 360 degrees. (Fig. 4) 2. Visualize which eye from the patient’s perspective. 3. Mark a point on the grid at 5BO and another at 2BU. 4. Draw a vertical line from the 5BO point and a horizontal line from the 2BU point. 5. The point of intersection of these two lines is the resultant of the two combined. 6. Now draw a line from this point to the center of the grid. 7. Using a mathematical equation known as The Pythagorean Theorem, the length of this resultant line can be calculated: Resultant^2 = 5^2+2^2 Resultant = ∆ 29 = 5.39 8. Now, using geometry, the angle between the resultant and the horizontal (xaxis) can be calculated: Sin angle = 2 ∆ 5.39 = 0.371 Sin angle = 21.8 degrees Resultant polar coordinates of 5BO and 2BU OS = 5.39∆ @ 21.8 degrees Don’t be concerned if this is too much math for comfort, or if you’re wondering what on earth is “Sin angle,” this is advanced optics. It will be handy when you sit for your Masters Certification, you will need to know how to determine resultant prism and how to resolve prism, and you will need an algebraic calculator. But for now, it is mentioned to illustrate the difference between the prescriber’s method and the lab method. Both are correct. 5BO and 2BU for the left eye, equals 5.39∆ @ 21.8 ∆. Although prism can be ordered in either polar coordinates or rectangular coordinates, your prism notation on your order should be precisely the same as the prescriber’s notation on the prescription. Why split prism using the rules of compounding? How does the brain handle prism? The eyes work as a team to produce binocular vision. When prismatic correction is placed in front of one eye, it affects both, the brain applies the effect binocularly. For this reason, the prism can be applied in just one eye or split between both, leading us to the topic of splitting prism. Note: Splitting prism should be done with the prescriber’s permission. Always check with the prescriber before splitting prism. Why do we want or need to split prism, and how is this beneficial? Answer: to balance the added weight and thickness resulting from prism, between the two lenses. Let’s look at the following prescription example: OD: 4.00 DS 8∆BD OS: 2.00 DS First, before even considering the prism, the right eye is going to be thicker at both the upper and lower edges. It’s twice the power of the left! Now, consider prism construction, it has a wide base. Prism will always add thickness in the direction of the base. Considering this, return to the above example, 8∆BD is going to add additional thickness to the lower edge of the right lens. The thickness disparity between the lenses will degrade lens cosmetics and increase the potential for distortion in the lens periphery. Here is where splitting prism power using the rules of compounding can be beneficial. It allows us to “split” the prescribed prism power between the two lenses instead of having one thick heavy lens with a visible imbalance in thickness between the right and left lenses. Splitting the 8∆BD by applying 4∆BD in the right eye and 4∆BU in the left eye will “share” the thickness of the prism between the two lenses. This is more cosmetically appealing than one thick lens with prism and one thin lens without. The prismatic effect of splitting the prisms using the rules of compounding has the same effect as if all of the prism is applied to the right eye. IMPORTANT RULES FOR SPLITTING PRISM • Always get permission from the prescriber. • Always adhere to compounding rules. • Always make sure the direction of the prism base as prescribed for the original eye remains the same. For example, OD: 16BD OS: PL OK to split as OD: 8BD and OS: 8BU NOT OD: 8BU and OS: 8BD What are some of the conditions for which prism is prescribed? First, what does prism do? It shifts the image in the direction of the apex. Prism is prescribed for various reasons, with the most common reason being muscle imbalance and eye alignment issues from strabismus. It is also prescribed for convergence issues, hemianopia and other conditions. The purpose of the prism is to alter the path of light from the object so that the images viewed by both left and right eyes correctly correspond to the visual axis of the eyes. As an example: If a right eye has esophoria (tendency to turn inward), then base out prism will bring the path of light from an object “inward” to be inline with the eye’s deviated visual axis. This allows the right eye to see the same object as the left eye and form an image on its retina, closer in similarity. Strabismus refers to misalignment, or deviation of the gaze or abnormal turning of the eyes, typically due to a muscular imbalance. The extraocular muscles of our eyes need to be able to maintain parallel alignment of each eye; both eyes need to be looking at the same thing in space and time. They control eye movement, in tandem, to ensure that any disparity between right and left retinal images is tolerable. This enables the brain to combine, or fuse, the separate images from two eyes into a single image—a process called Binocular Fusion. The most common use of prescribed prism is to compensate for strabismus, a condition where the extraocular muscles cannot maintain a balanced alignment of the two eyes. Strabismus is a broad medical term describing eye deviations that can be broken down into: phorias—a tendency for eye turn, deviation; and tropias—a definite eye turn, deviation. Eye deviations fall into two main categories: 1. Comitant—The most common in children. The deviation is constant, regardless of the direction of gaze, and 2. Incomitant—Deviation is always changing, depending on the direction of gaze. The prefix of a phoria or tropia indicates the direction of eye deviation. Eso = In (Esotropia or esophoria) Exo = Out (Exotropia or exophoria) Hyper = Up (Hypertropia or hyperphoria) Hypo = Down (Hypotropia or hypophoria) Strabismus can cause diplopia (Fig. 5). As stated earlier, extraocular muscles need to collaborate to make binocular fusion possible. If a muscular imbalance is present, resulting in strabismus, there can be an excessive disparity between the images each eye is sending to the brain, preventing binocular fusion. Ultimately, the brain “sees” and “reports” two separate images; hence, diplopia (double vision). When this happens during the years of eye development and is left untreated, the brain will often suppress (turn off) the weaker eye. The correctly functioning eye takes over, and input from the other eye is suppressed, a condition called amblyopia or lazy eye. In the past, it was thought that strabismus had to be treated roughly before age 7 to prevent permanent amblyopia. Now even adult amblyopes benefit from treatment. To review, to add prism to a lens has the effect of shifting the image of an object being viewed in the direction of the prism apex; thus, with eye deviations, it reduces the disparity of images formed on the left and right retinas. This enables the binocular fusion of the two retinal images in the brain. The primary use of prescribed prism is to aid binocular fusion, NOT to fix muscular alignment issues. Prescribed prism can also help improve quality of life for patients experiencing vision field loss due to neurological diseases such as a stroke or brain injury. These blind spots are known as Scotoma. Brain injuries or aneurysms, sometimes impact the occipital lobe of the brain, the area responsible for visual processing. These can result in visual field defects in specific quadrants, depending on the specific location of the injury. Fig. 6 illustrates the visual field defect a patient experienced after a stroke. As you see, the patient has lost vision in their left hemisphere of both eyes. When prisms are used to treat such conditions, the conventional rules for compounding and canceling prism are no longer employed. The objective is to “shift” the patient’s gaze in a direction to attempt to “look around” the defect and perceivably “widen” their field of vision, improving their quality of life. Example: In Fig. 6, the following prism may be prescribed: OD: BO OS: BI Generally, to accomplish the desired outcome, very high prism powers are required, which creates not only cosmetic problems but also a confusing visual environment in which objects unexpectedly appear and disappear from view. Aesthetics and the Impact of Frame Selection with Prism As a professional optician, always try to visualize the end product prior to fabrication. In a similar way to how lens thickness can be affected by PD, OC placement, frame dimensions and cylinder axis orientation, the base direction of the prescribed prism will also add thickness to the finished lens. For example, presented with the following prescription: OD: PL sph 5BIOS: PL sph 5BI. The thickest part of the lens will always be in the direction of the base. The base is the thickest part—makes sense? In this example, the lenses will be thickest at the nasal edge (BI OU). Knowing this helps with frame selection: • Keep frame PD as close as practically possible to the patient’s anatomical PD to minimize the necessary horizontal decentration. • Fitting the patient in a zyl frame without nosepads will not only cover up some of the lens edge, improving the cosmetics but also eliminate the need to adjust the nosepads around the thick nasal edges. • If anatomical features necessitate nosepads, the application of an edge roll at the nasal edge might help remedy the adjustment dilemma while also improving cosmetics. Occasionally, I’m faced with a moderate to high prescription and a patient electing to go “bigger” in frame size, despite my begging and pleading. In this case, all I can do is reiterate my recommendations and forewarn them of the distortion they may experience in the periphery. I hope that this helps prepare them and avoid a negative first impression of their new eyewear. Aspheric designs can help reduce the effect due to a flatter angle formed as the eye rotates away from the optical center of the lens. Antireflective coating: As stated earlier, prisms deviate light. It’s their job! Our real world presents the eyeglass wearer with omnidirectional light entering their lenses. Light entering the lens at oblique angles in an uncoated lens is going to scatter and reflect more from both the surface and internally, resulting in halos and ghost images that will be particularly apparent at night when driving into oncoming headlights. This effect will be exacerbated in the presence of a prescribed prism. The application of an antireflective treatment will minimize reflections and scatter to reduce eyestrain and fatigue, enhancing clarity and acuity—our primary objective. Nonprescribed prismatic effect of eyeglass lenses with centration errors (Fig.10): Prism occurs whenever there is a difference in lens thickness between two points on the lens. Because lenses with power always have a variation in lens thickness, prescription eyeglass lenses produce prismatic effects away from the optical center of the lens. At any point away from the optical center of the lens, a minus lens, which is thicker at the edge and thinner at the center, produces a prismatic effect with the prism base pointed away from the optical center. Conversely, a plus lens, which is thicker at the center and thinner at the edge, produces a prismatic effect with the prism base pointed in toward the optical center. The amount of prism at any point on a lens is directly proportional to the power of the lens and the distance from the optical center. Prentice rule is used to calculate the amount of prism present at any point in a lens. Prism = Decentration (distance) x Power ÷ 10 (Example: +6.00 D x 5 mm = 30 ÷ 10 = 3 ∆D. This formula gives you the amount of prism, but we need to know the base direction. If this is a right lens, then the amount of prism 5 mm below the OC is 3D D BU in a plus lens. If we want to know the amount of prism in this same lens, 5 mm out from the OC it is 3∆ D BI. A plus lens (Fig. 8) is constructed of base to base prisms, and because light deviates toward the base, it emerges from a plus lens converging: plus power (vergence). Plus lenses are a base in configuration. A minus lens (Fig. 9) is constructed of prisms arranged apex to apex, causing the light to bend toward the edges and emerge diverging: minus power (vergence). Minus lenses are a base out configuration. If you move a plus lens in front of your eye, you will see “against motion.” Do the same with a minus lens; you will see “with motion.” Prism: Good or Bad? What does prism do for our patients? As discussed earlier, it can be both beneficial if prescribed, but it can be detrimental if mistakenly induced in the patients’ ophthalmic lenses. How can prism be mistakenly induced? Prismatic effect from horizontal decentration errors (OCs and PDs not aligned): Through the optical center of the lens, rays of light do not deviate and therefore produce no prism. (OC = ZERO prism). As the distance from the optical center increases, rays of light will be deviated by increasing amounts. As illustrated in Fig. 10, misaligned PDs or OCs can induce unwanted prism, which can potentially cause vision problems and discomfort. These problems can present as distortion, headaches, a pulling sensation, eyestrain and fatigue and in severe cases, diplopia (double vision). ANSI standards indicate the following prism tolerance limits: horizontal prism < 2/3 ∆ D and vertical prism < 1/3 ∆ D In Part 2, we will address vertical prism imbalance in multifocal lenses and the effects of antimetropia or anisometropia. Prism Verification Now the job comes back from the lab, and it’s time to verify. You are verifying the correct prism amount and base direction, or you are determining the prism error in a lens. Take a deep breath, and here we go. • Mark the lens OC. • Viewing the lens through a lensometer, verify the prism through the OC, starting with the highest powered lens (most plus) first. • Very important: Set the platform position to check the highest powered lens and DO NOT move it. • Record vertical and horizontal prism present at this point in the first lens—the point of intersection of the middle line of the lensometer mires in each meridian. • Switch to the opposite lens, keeping lensometer platform height unchanged. • Verify prism. • Record vertical and horizontal prism. • Calculate net prism using rules for compounding and canceling prism and direction. Note: The above procedure works for single vision and lined multifocal designs. Verifying prism in a progressive addition lens (PAL): In a PAL, the prism can be verified only at the Prism Reference Point (PRP)–the point below the fitting cross and horizontally centered 17 mm in from the two engraved circles. This makes verifying prism in a PAL much easier than other lens design—it is definitive! 1. Locate engraved circles and mark them. 2. Position lens over PAL cutout template (or locate midpoint between the engraved circles). 3. Mark the PRP position (the dot below the fitting cross and centered between engraving marks). 4. Read vertical and horizontal prism through this point (PRP) for both lenses and calculate net error/imbalance or verify the prescribed prism amount. NOTE: Do not confuse the fitting cross with the PRP. Verify prism at the PRP and verify distance power at the distance reference point above the fitting cross. Do not be surprised if you find vertical prism ground at the PRP, despite not being prescribed. This is likely due to prism thinning. Prism thinning is a technique utilizing equal amounts of vertical prism in the same direction in each eye, usually base down, to create additional thickness in the lower portion of a PAL to accommodate the steepening base curves necessary to provide the increase in add power. It can also be used to reduce edge thickness in a high minus PAL. Since it is equal in both magnitude and direction and relatively minimal, it does not adversely affect a patient’s acuity. Ground prism resulting in no net effect is known as yoked prism and will be discussed in greater detail in Part 3. CONCLUSION Congratulations, you have completed this basic introduction to the world of prism. We will build on this foundation in Parts 2 and 3. I hope you are feeling less intimidated, and for those of you who can’t get enough, I hope I’ve whetted your appetite, and you are eagerly anticipating more. Either way, I hope you will all join me for the upcoming Parts 2 and 3 of The Spectrum of Prism Optics.
Find many great new & used options and get the best deals for Mechanical Iris Aperture Iris Diaphragm 11 Blades 2-50MM Condenser Camera Module at the best ...
Base In (BI), Base Out (BO), Base UP (BU) and Base Down (BD) or a combination of vertical and horizontal base directions.
Tien C-L, Lin H-Y, Cheng K-S, Chiang C-Y, Cheng C-Y. Design and Fabrication of a Cost-Effective Optical Notch Filter for Improving Visual Quality. Coatings. 2022; 12(1):19. https://doi.org/10.3390/coatings12010019
Do not be surprised if you find vertical prism ground at the PRP, despite not being prescribed. This is likely due to prism thinning. Prism thinning is a technique utilizing equal amounts of vertical prism in the same direction in each eye, usually base down, to create additional thickness in the lower portion of a PAL to accommodate the steepening base curves necessary to provide the increase in add power. It can also be used to reduce edge thickness in a high minus PAL. Since it is equal in both magnitude and direction and relatively minimal, it does not adversely affect a patient’s acuity. Ground prism resulting in no net effect is known as yoked prism and will be discussed in greater detail in Part 3.
Direct connection issues for footage offload: For most cameras: Power on the camera before plugging it in. Plug the cable in and you should see the USB symbol ...

Antireflective coating: As stated earlier, prisms deviate light. It’s their job! Our real world presents the eyeglass wearer with omnidirectional light entering their lenses. Light entering the lens at oblique angles in an uncoated lens is going to scatter and reflect more from both the surface and internally, resulting in halos and ghost images that will be particularly apparent at night when driving into oncoming headlights. This effect will be exacerbated in the presence of a prescribed prism. The application of an antireflective treatment will minimize reflections and scatter to reduce eyestrain and fatigue, enhancing clarity and acuity—our primary objective.
1. Create a grid showing 0 degree to 360 degrees. (Fig. 4) 2. Visualize which eye from the patient’s perspective. 3. Mark a point on the grid at 5BO and another at 2BU. 4. Draw a vertical line from the 5BO point and a horizontal line from the 2BU point. 5. The point of intersection of these two lines is the resultant of the two combined. 6. Now draw a line from this point to the center of the grid. 7. Using a mathematical equation known as The Pythagorean Theorem, the length of this resultant line can be calculated:
To review, to add prism to a lens has the effect of shifting the image of an object being viewed in the direction of the prism apex; thus, with eye deviations, it reduces the disparity of images formed on the left and right retinas. This enables the binocular fusion of the two retinal images in the brain. The primary use of prescribed prism is to aid binocular fusion, NOT to fix muscular alignment issues.
Oblique prism: Prisms are rarely just up, down, in or out. Most are oblique, which requires that a horizontal and vertical base direction be specified. Using rectangular coordinates will look like this example: OS 2D BI and 3D BU.
Notch filterQ factor
Congratulations, you have completed this basic introduction to the world of prism. We will build on this foundation in Parts 2 and 3. I hope you are feeling less intimidated, and for those of you who can’t get enough, I hope I’ve whetted your appetite, and you are eagerly anticipating more. Either way, I hope you will all join me for the upcoming Parts 2 and 3 of The Spectrum of Prism Optics.
In a PAL, the prism can be verified only at the Prism Reference Point (PRP)–the point below the fitting cross and horizontally centered 17 mm in from the two engraved circles. This makes verifying prism in a PAL much easier than other lens design—it is definitive!
1001 Optometry are a leading Australian group of optometrists and eyewear experts providing professional eye care with eye tests, glasses frames, ...
Abstract: This study presents a multilayer design and fabrication of an optical notch filter for enhancing visual quality. A cost-effective multilayer design of notch filter with low surface roughness and low residual stress is proposed. A 9-layer notch filter composed of SiO2 and Nb2O5 with a central wavelength of 480 nm is prepared by electron beam evaporation combined with ion-assisted deposition. The optical transmittance, residual stress, and surface morphology are measured by a UV/VIS/NIR spectrophotometer, Twyman-Green interferometer and field emission scanning electron microscopy (FE-SEM). The transmittance of the notch filter at the central wavelength is above 15%, and the average transmittance of the transmission band is about 80%. The residual stress of the notch filter is −0.235 GPa, and the root mean square surface roughness is 1.85 nm. For improving the visual quality, a good image contrast can be obtained by observing the microscopic image using the proposed notch filter. Keywords: notch filter; electron beam evaporation; ion-assisted deposition; surface roughness; residual stress
Adaptive Optics is another solution to atmospheric blurring. An Adaptive Optics system corrects the optical disturbances that light encounters as it traverses ...
Optical notch filterprice
How does the brain handle prism? The eyes work as a team to produce binocular vision. When prismatic correction is placed in front of one eye, it affects both, the brain applies the effect binocularly. For this reason, the prism can be applied in just one eye or split between both, leading us to the topic of splitting prism. Note: Splitting prism should be done with the prescriber’s permission. Always check with the prescriber before splitting prism. Why do we want or need to split prism, and how is this beneficial? Answer: to balance the added weight and thickness resulting from prism, between the two lenses.
• Record vertical and horizontal prism present at this point in the first lens—the point of intersection of the middle line of the lensometer mires in each meridian.
Nonprescribed prismatic effect of eyeglass lenses with centration errors (Fig.10): Prism occurs whenever there is a difference in lens thickness between two points on the lens. Because lenses with power always have a variation in lens thickness, prescription eyeglass lenses produce prismatic effects away from the optical center of the lens. At any point away from the optical center of the lens, a minus lens, which is thicker at the edge and thinner at the center, produces a prismatic effect with the prism base pointed away from the optical center. Conversely, a plus lens, which is thicker at the center and thinner at the edge, produces a prismatic effect with the prism base pointed in toward the optical center. The amount of prism at any point on a lens is directly proportional to the power of the lens and the distance from the optical center. Prentice rule is used to calculate the amount of prism present at any point in a lens.
4. Read vertical and horizontal prism through this point (PRP) for both lenses and calculate net error/imbalance or verify the prescribed prism amount.
Improve your science knowledge with free questions in "Applications of infrared waves" and thousands of other science skills.
• Fitting the patient in a zyl frame without nosepads will not only cover up some of the lens edge, improving the cosmetics but also eliminate the need to adjust the nosepads around the thick nasal edges.
A plus lens (Fig. 8) is constructed of base to base prisms, and because light deviates toward the base, it emerges from a plus lens converging: plus power (vergence). Plus lenses are a base in configuration.
Tien, C.-L.; Lin, H.-Y.; Cheng, K.-S.; Chiang, C.-Y.; Cheng, C.-Y. Design and Fabrication of a Cost-Effective Optical Notch Filter for Improving Visual Quality. Coatings 2022, 12, 19. https://doi.org/10.3390/coatings12010019
As a professional optician, always try to visualize the end product prior to fabrication. In a similar way to how lens thickness can be affected by PD, OC placement, frame dimensions and cylinder axis orientation, the base direction of the prescribed prism will also add thickness to the finished lens.
What does prism do for our patients? As discussed earlier, it can be both beneficial if prescribed, but it can be detrimental if mistakenly induced in the patients’ ophthalmic lenses. How can prism be mistakenly induced?
• Always get permission from the prescriber. • Always adhere to compounding rules. • Always make sure the direction of the prism base as prescribed for the original eye remains the same.
There are three major types of lenses used in lighthouse towers – fixed, flashing, and a combination of fixed and flashing. Flashing lights are the most ...
Notch filterschematic
Fig. 6 illustrates the visual field defect a patient experienced after a stroke. As you see, the patient has lost vision in their left hemisphere of both eyes. When prisms are used to treat such conditions, the conventional rules for compounding and canceling prism are no longer employed. The objective is to “shift” the patient’s gaze in a direction to attempt to “look around” the defect and perceivably “widen” their field of vision, improving their quality of life.
AR coatings improve the efficiency of optical instruments, enhance contrast in imaging devices, and reduces scattered light that can interfere with the optical ...
Here is where splitting prism power using the rules of compounding can be beneficial. It allows us to “split” the prescribed prism power between the two lenses instead of having one thick heavy lens with a visible imbalance in thickness between the right and left lenses. Splitting the 8∆BD by applying 4∆BD in the right eye and 4∆BU in the left eye will “share” the thickness of the prism between the two lenses. This is more cosmetically appealing than one thick lens with prism and one thin lens without. The prismatic effect of splitting the prisms using the rules of compounding has the same effect as if all of the prism is applied to the right eye.
ANSI standards indicate the following prism tolerance limits: horizontal prism < 2/3 ∆ D and vertical prism < 1/3 ∆ D
Notch filterdesign
RFnotch filter
Generally, to accomplish the desired outcome, very high prism powers are required, which creates not only cosmetic problems but also a confusing visual environment in which objects unexpectedly appear and disappear from view.
The thickest part of the lens will always be in the direction of the base. The base is the thickest part—makes sense? In this example, the lenses will be thickest at the nasal edge (BI OU).
What is a prism? Prism is a transparent triangular refracting medium with a base and apex (Fig. 1). Its apical (prism) angle determines its dioptric power. A prism of one prism diopter power (∆D) produces a 1 cm apparent displacement of an object located one meter away. Light entering the prism will deviate toward its base—however, the apparent image shifts (is displaced) toward the prism apex (Fig. 2). When used to correct for eye deviations, prism displaces the image of the object to align with the eye’s deviated visual axis. The image formed on the retina of the deviated eye will now be similar to that formed on the retina of the nondeviated eye so that binocular fusion occurs, and the brain creates one single focused image by fusing the left and right retinal images. A prisms’ ability to deflect light is measured in prism diopters, denoted as ∆D, the Greek capital letter delta symbol. A 1D prism will displace an image 1 cm at a distance of 1 meter. Note: A prism diopter and lens diopter is different. Prism diopters change the path of light. A lens diopter is a measure of focal power (vergence), its ability to converge or diverge light to shorten or lengthen the focal length. As you already know, lens dioptric power is the inverse of its focal length in meters. (1/f=D) But this is another lesson for another course; today, we are dealing with prism diopter. Prism Convention There are two methods used for specifying prism called rectangular coordinates (Fig. 3) and polar coordinates. The prescriber’s method uses rectangular coordinates of horizontal and vertical measurements. The laboratory reference system uses a polar coordinate system of specifying the direction in degrees. Prescribing doctors and opticians in the U.S. typically use rectangular, while optical labs and European countries use polar coordinates. Rectangular Coordinates Base In (BI), Base Out (BO), Base UP (BU) and Base Down (BD) or a combination of vertical and horizontal base directions. COMPOUNDING OR CANCELING PRISMS Rules for horizontal or lateral prism: Compounding effect (prismatic effects of each eye are additive)—The prism bases must be in the same direction OU. For example, BI OU. Canceling Effect (prismatic effects are subtractive)—The prism bases must be in opposite directions OU. For example, BI and BO. Rules for vertical prism: Compounding effect—The prism bases must be in opposite directions OU. For example, BU and BD. Canceling effect—The prism bases must be in the same direction OU. For example, BU OU. Oblique prism: Prisms are rarely just up, down, in or out. Most are oblique, which requires that a horizontal and vertical base direction be specified. Using rectangular coordinates will look like this example: OS 2D BI and 3D BU. Rectangular coordinates can be converted to polar coordinates to determine the resultant prism. Labs typically use the 360 or 180 degree reference system to determine prism base direction. This means that the multiple base directions of the rectangular system are not used. Instead, the prism is resolved into the net amount of prism and degree of placement. What follows are the steps for converting rectangular coordinates to polar coordinates using the 360 degree lab reference system. Example: OS 5BO 2BU (Fig. 4) 1. Create a grid showing 0 degree to 360 degrees. (Fig. 4) 2. Visualize which eye from the patient’s perspective. 3. Mark a point on the grid at 5BO and another at 2BU. 4. Draw a vertical line from the 5BO point and a horizontal line from the 2BU point. 5. The point of intersection of these two lines is the resultant of the two combined. 6. Now draw a line from this point to the center of the grid. 7. Using a mathematical equation known as The Pythagorean Theorem, the length of this resultant line can be calculated: Resultant^2 = 5^2+2^2 Resultant = ∆ 29 = 5.39 8. Now, using geometry, the angle between the resultant and the horizontal (xaxis) can be calculated: Sin angle = 2 ∆ 5.39 = 0.371 Sin angle = 21.8 degrees Resultant polar coordinates of 5BO and 2BU OS = 5.39∆ @ 21.8 degrees Don’t be concerned if this is too much math for comfort, or if you’re wondering what on earth is “Sin angle,” this is advanced optics. It will be handy when you sit for your Masters Certification, you will need to know how to determine resultant prism and how to resolve prism, and you will need an algebraic calculator. But for now, it is mentioned to illustrate the difference between the prescriber’s method and the lab method. Both are correct. 5BO and 2BU for the left eye, equals 5.39∆ @ 21.8 ∆. Although prism can be ordered in either polar coordinates or rectangular coordinates, your prism notation on your order should be precisely the same as the prescriber’s notation on the prescription. Why split prism using the rules of compounding? How does the brain handle prism? The eyes work as a team to produce binocular vision. When prismatic correction is placed in front of one eye, it affects both, the brain applies the effect binocularly. For this reason, the prism can be applied in just one eye or split between both, leading us to the topic of splitting prism. Note: Splitting prism should be done with the prescriber’s permission. Always check with the prescriber before splitting prism. Why do we want or need to split prism, and how is this beneficial? Answer: to balance the added weight and thickness resulting from prism, between the two lenses. Let’s look at the following prescription example: OD: 4.00 DS 8∆BD OS: 2.00 DS First, before even considering the prism, the right eye is going to be thicker at both the upper and lower edges. It’s twice the power of the left! Now, consider prism construction, it has a wide base. Prism will always add thickness in the direction of the base. Considering this, return to the above example, 8∆BD is going to add additional thickness to the lower edge of the right lens. The thickness disparity between the lenses will degrade lens cosmetics and increase the potential for distortion in the lens periphery. Here is where splitting prism power using the rules of compounding can be beneficial. It allows us to “split” the prescribed prism power between the two lenses instead of having one thick heavy lens with a visible imbalance in thickness between the right and left lenses. Splitting the 8∆BD by applying 4∆BD in the right eye and 4∆BU in the left eye will “share” the thickness of the prism between the two lenses. This is more cosmetically appealing than one thick lens with prism and one thin lens without. The prismatic effect of splitting the prisms using the rules of compounding has the same effect as if all of the prism is applied to the right eye. IMPORTANT RULES FOR SPLITTING PRISM • Always get permission from the prescriber. • Always adhere to compounding rules. • Always make sure the direction of the prism base as prescribed for the original eye remains the same. For example, OD: 16BD OS: PL OK to split as OD: 8BD and OS: 8BU NOT OD: 8BU and OS: 8BD What are some of the conditions for which prism is prescribed? First, what does prism do? It shifts the image in the direction of the apex. Prism is prescribed for various reasons, with the most common reason being muscle imbalance and eye alignment issues from strabismus. It is also prescribed for convergence issues, hemianopia and other conditions. The purpose of the prism is to alter the path of light from the object so that the images viewed by both left and right eyes correctly correspond to the visual axis of the eyes. As an example: If a right eye has esophoria (tendency to turn inward), then base out prism will bring the path of light from an object “inward” to be inline with the eye’s deviated visual axis. This allows the right eye to see the same object as the left eye and form an image on its retina, closer in similarity. Strabismus refers to misalignment, or deviation of the gaze or abnormal turning of the eyes, typically due to a muscular imbalance. The extraocular muscles of our eyes need to be able to maintain parallel alignment of each eye; both eyes need to be looking at the same thing in space and time. They control eye movement, in tandem, to ensure that any disparity between right and left retinal images is tolerable. This enables the brain to combine, or fuse, the separate images from two eyes into a single image—a process called Binocular Fusion. The most common use of prescribed prism is to compensate for strabismus, a condition where the extraocular muscles cannot maintain a balanced alignment of the two eyes. Strabismus is a broad medical term describing eye deviations that can be broken down into: phorias—a tendency for eye turn, deviation; and tropias—a definite eye turn, deviation. Eye deviations fall into two main categories: 1. Comitant—The most common in children. The deviation is constant, regardless of the direction of gaze, and 2. Incomitant—Deviation is always changing, depending on the direction of gaze. The prefix of a phoria or tropia indicates the direction of eye deviation. Eso = In (Esotropia or esophoria) Exo = Out (Exotropia or exophoria) Hyper = Up (Hypertropia or hyperphoria) Hypo = Down (Hypotropia or hypophoria) Strabismus can cause diplopia (Fig. 5). As stated earlier, extraocular muscles need to collaborate to make binocular fusion possible. If a muscular imbalance is present, resulting in strabismus, there can be an excessive disparity between the images each eye is sending to the brain, preventing binocular fusion. Ultimately, the brain “sees” and “reports” two separate images; hence, diplopia (double vision). When this happens during the years of eye development and is left untreated, the brain will often suppress (turn off) the weaker eye. The correctly functioning eye takes over, and input from the other eye is suppressed, a condition called amblyopia or lazy eye. In the past, it was thought that strabismus had to be treated roughly before age 7 to prevent permanent amblyopia. Now even adult amblyopes benefit from treatment. To review, to add prism to a lens has the effect of shifting the image of an object being viewed in the direction of the prism apex; thus, with eye deviations, it reduces the disparity of images formed on the left and right retinas. This enables the binocular fusion of the two retinal images in the brain. The primary use of prescribed prism is to aid binocular fusion, NOT to fix muscular alignment issues. Prescribed prism can also help improve quality of life for patients experiencing vision field loss due to neurological diseases such as a stroke or brain injury. These blind spots are known as Scotoma. Brain injuries or aneurysms, sometimes impact the occipital lobe of the brain, the area responsible for visual processing. These can result in visual field defects in specific quadrants, depending on the specific location of the injury. Fig. 6 illustrates the visual field defect a patient experienced after a stroke. As you see, the patient has lost vision in their left hemisphere of both eyes. When prisms are used to treat such conditions, the conventional rules for compounding and canceling prism are no longer employed. The objective is to “shift” the patient’s gaze in a direction to attempt to “look around” the defect and perceivably “widen” their field of vision, improving their quality of life. Example: In Fig. 6, the following prism may be prescribed: OD: BO OS: BI Generally, to accomplish the desired outcome, very high prism powers are required, which creates not only cosmetic problems but also a confusing visual environment in which objects unexpectedly appear and disappear from view. Aesthetics and the Impact of Frame Selection with Prism As a professional optician, always try to visualize the end product prior to fabrication. In a similar way to how lens thickness can be affected by PD, OC placement, frame dimensions and cylinder axis orientation, the base direction of the prescribed prism will also add thickness to the finished lens. For example, presented with the following prescription: OD: PL sph 5BIOS: PL sph 5BI. The thickest part of the lens will always be in the direction of the base. The base is the thickest part—makes sense? In this example, the lenses will be thickest at the nasal edge (BI OU). Knowing this helps with frame selection: • Keep frame PD as close as practically possible to the patient’s anatomical PD to minimize the necessary horizontal decentration. • Fitting the patient in a zyl frame without nosepads will not only cover up some of the lens edge, improving the cosmetics but also eliminate the need to adjust the nosepads around the thick nasal edges. • If anatomical features necessitate nosepads, the application of an edge roll at the nasal edge might help remedy the adjustment dilemma while also improving cosmetics. Occasionally, I’m faced with a moderate to high prescription and a patient electing to go “bigger” in frame size, despite my begging and pleading. In this case, all I can do is reiterate my recommendations and forewarn them of the distortion they may experience in the periphery. I hope that this helps prepare them and avoid a negative first impression of their new eyewear. Aspheric designs can help reduce the effect due to a flatter angle formed as the eye rotates away from the optical center of the lens. Antireflective coating: As stated earlier, prisms deviate light. It’s their job! Our real world presents the eyeglass wearer with omnidirectional light entering their lenses. Light entering the lens at oblique angles in an uncoated lens is going to scatter and reflect more from both the surface and internally, resulting in halos and ghost images that will be particularly apparent at night when driving into oncoming headlights. This effect will be exacerbated in the presence of a prescribed prism. The application of an antireflective treatment will minimize reflections and scatter to reduce eyestrain and fatigue, enhancing clarity and acuity—our primary objective. Nonprescribed prismatic effect of eyeglass lenses with centration errors (Fig.10): Prism occurs whenever there is a difference in lens thickness between two points on the lens. Because lenses with power always have a variation in lens thickness, prescription eyeglass lenses produce prismatic effects away from the optical center of the lens. At any point away from the optical center of the lens, a minus lens, which is thicker at the edge and thinner at the center, produces a prismatic effect with the prism base pointed away from the optical center. Conversely, a plus lens, which is thicker at the center and thinner at the edge, produces a prismatic effect with the prism base pointed in toward the optical center. The amount of prism at any point on a lens is directly proportional to the power of the lens and the distance from the optical center. Prentice rule is used to calculate the amount of prism present at any point in a lens. Prism = Decentration (distance) x Power ÷ 10 (Example: +6.00 D x 5 mm = 30 ÷ 10 = 3 ∆D. This formula gives you the amount of prism, but we need to know the base direction. If this is a right lens, then the amount of prism 5 mm below the OC is 3D D BU in a plus lens. If we want to know the amount of prism in this same lens, 5 mm out from the OC it is 3∆ D BI. A plus lens (Fig. 8) is constructed of base to base prisms, and because light deviates toward the base, it emerges from a plus lens converging: plus power (vergence). Plus lenses are a base in configuration. A minus lens (Fig. 9) is constructed of prisms arranged apex to apex, causing the light to bend toward the edges and emerge diverging: minus power (vergence). Minus lenses are a base out configuration. If you move a plus lens in front of your eye, you will see “against motion.” Do the same with a minus lens; you will see “with motion.” Prism: Good or Bad? What does prism do for our patients? As discussed earlier, it can be both beneficial if prescribed, but it can be detrimental if mistakenly induced in the patients’ ophthalmic lenses. How can prism be mistakenly induced? Prismatic effect from horizontal decentration errors (OCs and PDs not aligned): Through the optical center of the lens, rays of light do not deviate and therefore produce no prism. (OC = ZERO prism). As the distance from the optical center increases, rays of light will be deviated by increasing amounts. As illustrated in Fig. 10, misaligned PDs or OCs can induce unwanted prism, which can potentially cause vision problems and discomfort. These problems can present as distortion, headaches, a pulling sensation, eyestrain and fatigue and in severe cases, diplopia (double vision). ANSI standards indicate the following prism tolerance limits: horizontal prism < 2/3 ∆ D and vertical prism < 1/3 ∆ D In Part 2, we will address vertical prism imbalance in multifocal lenses and the effects of antimetropia or anisometropia. Prism Verification Now the job comes back from the lab, and it’s time to verify. You are verifying the correct prism amount and base direction, or you are determining the prism error in a lens. Take a deep breath, and here we go. • Mark the lens OC. • Viewing the lens through a lensometer, verify the prism through the OC, starting with the highest powered lens (most plus) first. • Very important: Set the platform position to check the highest powered lens and DO NOT move it. • Record vertical and horizontal prism present at this point in the first lens—the point of intersection of the middle line of the lensometer mires in each meridian. • Switch to the opposite lens, keeping lensometer platform height unchanged. • Verify prism. • Record vertical and horizontal prism. • Calculate net prism using rules for compounding and canceling prism and direction. Note: The above procedure works for single vision and lined multifocal designs. Verifying prism in a progressive addition lens (PAL): In a PAL, the prism can be verified only at the Prism Reference Point (PRP)–the point below the fitting cross and horizontally centered 17 mm in from the two engraved circles. This makes verifying prism in a PAL much easier than other lens design—it is definitive! 1. Locate engraved circles and mark them. 2. Position lens over PAL cutout template (or locate midpoint between the engraved circles). 3. Mark the PRP position (the dot below the fitting cross and centered between engraving marks). 4. Read vertical and horizontal prism through this point (PRP) for both lenses and calculate net error/imbalance or verify the prescribed prism amount. NOTE: Do not confuse the fitting cross with the PRP. Verify prism at the PRP and verify distance power at the distance reference point above the fitting cross. Do not be surprised if you find vertical prism ground at the PRP, despite not being prescribed. This is likely due to prism thinning. Prism thinning is a technique utilizing equal amounts of vertical prism in the same direction in each eye, usually base down, to create additional thickness in the lower portion of a PAL to accommodate the steepening base curves necessary to provide the increase in add power. It can also be used to reduce edge thickness in a high minus PAL. Since it is equal in both magnitude and direction and relatively minimal, it does not adversely affect a patient’s acuity. Ground prism resulting in no net effect is known as yoked prism and will be discussed in greater detail in Part 3. CONCLUSION Congratulations, you have completed this basic introduction to the world of prism. We will build on this foundation in Parts 2 and 3. I hope you are feeling less intimidated, and for those of you who can’t get enough, I hope I’ve whetted your appetite, and you are eagerly anticipating more. Either way, I hope you will all join me for the upcoming Parts 2 and 3 of The Spectrum of Prism Optics.
Rules for horizontal or lateral prism: Compounding effect (prismatic effects of each eye are additive)—The prism bases must be in the same direction OU. For example, BI OU. Canceling Effect (prismatic effects are subtractive)—The prism bases must be in opposite directions OU. For example, BI and BO.
The content contained on this website is for informational purposes only. The content is not intended to be a substitute for professional advice.Reliance on any information provided in this article is solely at your own risk.
Don’t be concerned if this is too much math for comfort, or if you’re wondering what on earth is “Sin angle,” this is advanced optics. It will be handy when you sit for your Masters Certification, you will need to know how to determine resultant prism and how to resolve prism, and you will need an algebraic calculator. But for now, it is mentioned to illustrate the difference between the prescriber’s method and the lab method. Both are correct. 5BO and 2BU for the left eye, equals 5.39∆ @ 21.8 ∆. Although prism can be ordered in either polar coordinates or rectangular coordinates, your prism notation on your order should be precisely the same as the prescriber’s notation on the prescription.
Infrared light is an electromagnetic radiation between microwave and visible light, with a wavelength of 0.78 ∼ 1000 μm, including near-infrared (NIR, 0.78 ∼ ...
Tien C-L, Lin H-Y, Cheng K-S, Chiang C-Y, Cheng C-Y. Design and Fabrication of a Cost-Effective Optical Notch Filter for Improving Visual Quality. Coatings. 2022; 12(1):19. https://doi.org/10.3390/coatings12010019
There are two methods used for specifying prism called rectangular coordinates (Fig. 3) and polar coordinates. The prescriber’s method uses rectangular coordinates of horizontal and vertical measurements. The laboratory reference system uses a polar coordinate system of specifying the direction in degrees. Prescribing doctors and opticians in the U.S. typically use rectangular, while optical labs and European countries use polar coordinates.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess.



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500