
Contact Lens Conversion Calculator - contact lens finder
All the patients in the contralateral and bilateral IC-8 IOL study achieved good vision, satisfaction, and low visual symptoms even if the lens was implanted irrespective of eye dominance.[16] The bilateral group extended depth of focus by 0.25 D, had 0.5 to one line greater binocular UIVA and UNVA, higher spectacle independence, and better overall satisfaction than the contralateral group. In another study, bilateral IC-8 IOL implantation resulted in higher curves in the defocus curve analysis while maintaining the same peak as those contralaterally implanted with the IC-8 IOL.[15]
In the bilateral XtraFocus device study, darkening vision complaints were reported in 18.8% after implantation in the first eye causing exclusion from XtraFocus device placement in the fellow eye.[33] In another study, the patient who had XtraFocus explantation had complete resolution of the persistent glare and halos after device removal.[32] Dilated infrared photography showed no interlenticular opacification for up to 4 years postoperatively.[6] The authors noted that this was possibly due to the posterior concave shape of the IOL that reduced contact with the other IOL inside the bag while its central hole allowed exit of lens cells through aqueous movement.[6] Nd:YAG laser posterior capsulotomy was done with no difficulty using a Peyman contact lens to improve focus and if needed, the capsulotomy could be sized larger than the pinhole by modifying the patient gaze.[6,33]
The Lynx L6-4 Interior Light Bar with linear 1 optics features 24 Gen. IV LEDs, 30 unique flash patterns, 4 suction cups, and is waterproof for exterior ...
UNIVERSAL BOWENS MOUNTThe Light Dome SE is designed to grow along with your creative journey. Featuring the most universal mount possible, we created this modifier to be versatile and compatible with not only the Amaran 100d/x and Amaran 200d/x, but also the Aputure 120d, Aputure 300d, and even many other third-party Bowens Mount lights.
aFirst author and year study was published, bMonofocal aspheric IOL, cBilateral AT Lisa Tritoric IOL, † Schojai et al.[12] monocular and binocular UDVA measured under photopic light conditions, ‡Target refraction −0.75 D for the majority[5,12,13,28], except for Shajari et al.[13] and all DE (target of plano), Dick et al.[14,15] and Ang[16] NDE (−0.5 D to −0.75 D), and Agarwal[29] OD, OS (0 D to ±0.5 D). B=Bilateral, C=Contralateral, DE=Dominant eye, J=Jaeger, m=Months, NA=Not available, NDE=Nondominant eye, OD=Right eye, OS=Left eye, px=Patient, SE=Spherical equivalent, UDVA=Uncorrected distance visual acuity, UIVA=Uncorrected intermediate visual acuity, UNVA=Uncorrected near visual acuity, y/o=Years old, IOL=Intraocular lens
Aputure
Patients implanted with the XtraFocus device hardly noticed the Pulfrich effect or the distortion of perceived object motion due to differences in interocular retinal luminance such as when a pendulum moving laterally appears to be moving in an elliptical pattern.[8] The authors surmised that the retinal luminance difference between the eye implanted with the XtraFocus and the fellow eye may not have been significant enough for the patients to notice the optical phenomenon and that their poorer optical quality from the high corneal aberrations may have played a part. The brightness seen by the patients was also not reduced to the amount expected with the XtraFocus device partly due to the Stiles-Crawford effect, which implies that smaller pupils can achieve per unit light of energy a higher degree of visual response compared to larger pupils.[8]
A goniospectrophotometer is an instrument that measures flux, either reflected or transmitted, as a function of illumination and collection angle per ...
Shajari et al. investigated the IC-8 IOL in eyes with severe corneal irregularities, most of whom preoperatively had early cataracts or none.[13] Despite this, 94% had better postoperative CDVA compared to preoperatively, were able to perform daily tasks better, and had high satisfaction rates with the IC-8 IOL. Agarwal et al. implanted the IC-8 IOL on three patients with irregular astigmatism who had bilateral radial keratotomy from more than 20 to 30 years ago.[29] Stereopsis was maintained in the IC-8 IOL eyes, majority did not need spectacles, and no visual disturbances were reported despite the high preoperative total corneal higher-order aberrations (HOAs) and coma scores, the lowest being 0.210 μm and 0.098 μm respectively.[29]
We strive to maintain accuracy and have the most up to date information on our website. Should the website contents contain any accidental errors, we cannot be held accountable and will not accept any orders or payments based on an incorrect price, product information or product images.
20€ in einer Filiale oder im Onlineshop der Dirk Rossmann GmbH und bei Einkauf in der Filiale das Scannenlassen des QR-Codes in der App beim Kauf an der Kasse ...
Our products: Armored cable (Type AC, Type MC), metallic, non-metallic, and liquidtight flexible metal conduits, specialty cables, cable and conduit ...
Small aperture optics work by blocking unfocused peripheral light rays while allowing central light rays to focus on the retina. This pinhole effect creates an extended depth of focus and has been used in presbyopia correction, improving intermediate and near vision without markedly affecting distance vision. Another beneficial effect of small aperture optics is reducing aberrations caused by irregular corneas or irregular pupils. The first small aperture surgical device was the Kamra corneal inlay used on the nondominant eyes of presbyopic emmetropes. The pinhole concept was also adapted into the IC-8 intraocular lens (IOL) for presbyopia correction during cataract surgery and by the XtraFocus piggyback device to lessen unwanted aberrations in eyes with irregular corneas or pupils. The IC-8 IOL can be placed monocularly or binocularly with mini-monovision for further near vision improvement. The XtraFocus piggyback device can be placed either in the sulcus or capsular bag. The aim of this literature review is to synthesize evidence on the efficacy, safety, and patient-reported outcomes on surgical devices utilizing small aperture optics. A comprehensive search on PubMed was conducted with the keywords “small aperture optics,” “small aperture corneal inlay,” “small aperture IOL,” “Kamra corneal inlay,” “IC-8 IOL,” and “XtraFocus.” In this review, we describe the progression of small aperture surgical devices, patient criteria, visual outcomes, complications, satisfaction, and recommendations for surgical success.
TRAVEL LIGHTWeighing in at roughly 1kg (2.2lbs), the Light Dome SE is one of the most portable lighting modifiers ever. Every Light Dome SE also ships with its own carrying bag to guarantee that no matter where your shoot takes you, your gear will arrive safe & sound, and ready-to-go.
CIRCULAR DESIGNWhen filming any subject, reflections are bound to occur. Many are desirable like the catch light of a model’s eyes. Using 16 fiberglass rods, the Light Dome SE guarantees beautiful, circular reflections that are always pleasing to the eye.
In the contralateral versus bilateral IC-8 IOL implantation study by Ang, if the patient did not achieve the desired near or intermediate vision with the first IC-8 IOL eye that was targeted for myopia, the second IC-8 IOL eye was targeted for more myopia instead of the previously planned emmetropia.[16] This study showed that optimization of refractive targets resulted in excellent visual acuities with the IC-8 IOL across all distances and high patient satisfaction. Ocular surface disorders must be treated well preoperatively and postoperatively to maximize the IC-8 IOL.[14] Patients must be counseled that some may experience postoperative dysphotopsias which often resolve eventually but might persist in a few cases.[5] The full benefits from the IC-8 IOL are often experienced after neuroadaptation.[5]
At Zenni Canada, we believe that stylish, high-quality prescribed glasses should be accessible to all. As a leading online glasses company since 2003, we've ...
The IC-8 IOL was found to be effective, safe, and received good patient satisfaction feedback in terms of presbyopia correction and spectacle independence when implanted monocularly or binocularly.[5,12,13,14,15,16,28,29] Even if the IC-8 IOL has no cylinder correction in its design, patients with up to 1.5 D of corneal astigmatism can benefit whether in virgin corneas or post-refractive surgery patients who may be at risk for postoperative refractive surprises.[16] Hooshmand et al. found that patients with ocular comorbidities such as age-related macular degeneration, epiretinal membrane, and marked corneal HOAs were satisfied with their significant gain in extended depth of focus after IC-8 IOL implantation.[5] Patients deemed unsuitable for multifocal IOLs may benefit from the IC-8 small aperture IOL.[5]
Dick et al. reported that mean UDVA was better in the monofocal IOL eyes by half a line while the IC-8 IOL eyes had better mean UIVA and UNVA by two lines and three lines, respectively.[14] Mean binocular defocus curves with distance correction had visual acuity of 20/32 or better over a range of about 2.15 D of defocus. Functional near vision range was extended by an additional diopter using −0.75 D target-corrected defocus curves without loss of distance vision compared with the distance-corrected defocus curves.
Jun 4, 2024 — What is the magnification of a beam expander with focal lengths 100 mm and 15 mm? ... To find the magnifying power, take the inverse of the ...
PCO develops in all types of IOLs, including the IC-8. A modified capsulotomy technique was developed due to the presence of the small aperture mask. Nd:YAG capsulotomy was successfully performed using an omega pattern of firing around the IOL mask, leaving the posterior capsulotomy connected at the bottom to allow the capsule to float down or tilt backward.[16] Another variation is completely disconnecting the PCO 360°then firing extra shots through the small aperture to dislodge the capsule that may remain attached to the optic.
Light dome150
A decrease in aperture diameter causes an increase in the depth of field or the distance in front of and behind the object of regard that appears in focus. However, if the decrease in the aperture size is too much, the visual acuity suffers due to increased diffraction and decreased light transmission.[34] The balance between these was found through computer modeling and was applied in the creation of small aperture optics devices.[34] Surgical devices that utilize small aperture optics have proven their usefulness as extended depth of focus tools. The implanted eye can see well at all distances as the blur circle is reduced, the conoid of Sturm narrowed, and the effect of ocular aberrations minimized.[1,8,17]
Dr. Ang was a principal investigator for clinical studies conducted on the Kamra corneal inlay and IC-8 intraocular lens. Dr. Ang and the co-authors have no financial interest related to this submitted work.
In comparison to classic monovision wherein one eye is made myopic and loses distance vision, eyes implanted with a small aperture device gain intermediate and near vision and can still be used for distance vision.[14] Compared to monovision mean results, the UDVA results were better in both the Kamra corneal inlay and the IC-8 IOL.[10,24,29,35] Some stereoacuity is lost with traditional monovision because of the anisometropia but stereoacuity is maintained with the −0.75 D mini-monovision used with small aperture devices.[10,29,35] Small aperture devices are more forgiving in terms of refractive targeting because of their increased depth of focus. Furthermore, the Kamra corneal inlay, IC-8 IOL, and XtraFocus device have been used in combination with other procedures or as a rescue procedure.
MULTIPLE DIFFUSIONSIn order to be creative, an artist must have options. The Light Dome SE includes two types of diffusion fabric, one light (1.5 stops) and one heavy (2.5 stops), allowing users to pick and choose the perfect level of softness for every subject that they film.
2024515 — A macro zoom lens is one in which the magnification can be changed continuously and the focal length is constant (does not change).
High rates of binocular UDVA and UIVA of 20/25 or better and UNVA of J3 or better were achieved in the IC-8 IOL patients [Table 5].[5,12,14,15,16,28] The first IC-8 IOL publication by Grabner, Ang, and Vilupuru reported mean UDVA, UIVA, and UNVA monocular implantation results of 20/20, 20/25, and J2, respectively, while binocular values were 20/20, 20/21, and J2, respectively.[28] The mean satisfaction score was 5.1 (1 very dissatisfied, 7 very satisfied).[28]
FLATTERING SOFT LIGHTWhen it comes to filming faces, creating a soft quality of light is the key to making any subject look flattering. With its wide 33.5-inch diameter, the Light Dome SE creates a beautiful soft light specially designed to blanket your subject, hide blemishes, and make everyone look stunning on-camera.
The statistically significant improvements after XtraFocus device implantation for UDVA and CDVA from baseline values were sustained up to 4 years of follow-up.[6] In the study by Ho et al., all their patients had poor vision or glare preoperatively due to a standalone iris defect or coexisting irregular astigmatism and iris defect.[32] After XtraFocus implantation, 90.9% had better UDVA and 72.7% reported satisfaction with the improved vision or lessened glare.[32] The refractive and visual acuity outcomes of the XtraFocus IOL publications are summarized in [Table 6].
Small aperture surgical devices accomplished reasonable levels of efficacy, safety, spectacle independence, and satisfaction. The long-term biocompatibility of the Kamra corneal inlay has limited its clinical use. The IC-8 IOL is a promising technology for presbyopia correction during cataract surgery. The EDOF capability provides excellent outcomes for monocular or binocular implantation, the latter further improving near and intermediate vision. Aside from presbyopia, the IC-8 IOL offers an alternative solution for eyes with corneal astigmatism up to 1.50 D and eyes with complex corneas who have had previous corneal refractive surgery or have corneal irregularities. The XtraFocus piggyback device is the ideal rescue solution for pseudophakic eyes suffering from debilitating best-corrected vision arising from iris defects or corneal irregular astigmatism due to keratoconus, ectasia, trauma, or prior corneal transplant.
Small aperture optics work by increasing depth of focus as unfocused peripheral light rays are blocked by an opaque mask while only the central light rays can pass through. This pinhole effect narrows the retinal blur circle, resulting in near and intermediate vision improvement without much effect on distance vision. The first commercially approved small aperture surgical device is the Kamra corneal inlay (CorneaGen, Seattle, Washington, USA), an opaque ring-shaped device. It is the only corneal implant that uses small aperture optics to correct presbyopia. Accommodation is gradually lost due to aging, but accommodation loss also occurs after cataract surgery when a monofocal intraocular lens (IOL) is implanted. An annular mask similar to the Kamra corneal inlay was embedded inside a monofocal IOL to create the small aperture IC-8 IOL (Acufocus Inc., Irvine, California, USA). It employs the same extended depth of focus mechanism as the Kamra corneal inlay for presbyopia correction but located at the lens plane and with the ability to correct refractive errors.
There have been three generations of the Kamra corneal inlay, the ACI7000, ACI7000PD, and the latest being the ACI7000PDT, with PDT standing for pattern, darker, and thinner.[9] The first generation had 1600 microperforations, 7.1% light transmission, and 10 μm thickness.[18] The second generation Kamra inlay was made darker with 5% light transmission but with more microperforations at 8400 while the third generation incorporated the thinner design of 5 μm.[9] The increased number of microperforations in the latest version of the inlay improved nutritional flow through the cornea, the thinner design resulted in less biomechanical changes, and the decreased light transmission helped reduce visual symptoms.
Uncorrected visual acuities remained the same in the IC-8 IOL eyes up to 1.5 D of residual astigmatism.[5,14] As for induced astigmatism, Ang investigated this across three axes (with-the-rule, against-the-rule, and oblique) for three types of IOLs.[30] When all astigmatic axes were combined, no more than one line of loss from baseline visual acuity occurred with induced astigmatic defocus of up to 1.40 D for the IC-8 IOL small aperture patients, 1.00 D for the enVista IOL (Bausch and Lomb, Rochester, NY, USA) monofocal patients, and 0.70 D for the FineVision IOL (PhysIOL SA, Liege, Belgium) and AT Lisa IOL (Carl Zeiss AG, Jena, Germany) trifocal patients.[30] This greater tolerance for astigmatism with the IC-8 IOL translates to simplified IOL implantation compared to toric IOLs, wherein alignment is crucial and IOL rotation is a possibility. Additional procedures for astigmatic management such as limbal relaxing incisions may be reduced. Furthermore, there is less risk for dissatisfaction when an IC-8 IOL is used compared to a multifocal or trifocal IOL if there is residual astigmatism of −0.75 D to −1.5 D.
Irregular corneas or irregular pupils cause unwanted aberrations and patients who suffer from these conditions can benefit from the aberration-reducing capability of small aperture optics. The Xtrafocus small Aperture piggyback device (Morcher, Stuttgart, Germany) is black and shaped like a C-loop IOL. It is implanted in the sulcus or inside the capsular bag. Both the Xtrafocus device and the IC-8 IOL can filter out unwanted aberrations, thereby improving the overall vision of the pseudophakic eye. In this review, we condense published literature and describe the patient selection, surgical techniques, postoperative outcomes, and the current status of these three small aperture surgical devices, namely the Kamra corneal inlay, IC-8 IOL, and XtraFocus piggyback device.
aFirst author and year study was published, b1st generation Kamra corneal inlay: ACI7000, c2nd generation Kamra corneal inlay: ACI7000PD, d3rd generation Kamra corneal inlay: ACI7000PDT, eAll LASIK patients except for Moshirfar 2018[23] who also had PRK patients; included hyperopic, emmetropic, and myopic patients except for Tomita and Waring 2015[21] and Abdul Fattah et al., 2020[24] who only had hyperopic patients, fPatients subgrouped by age: I. 45-49 years old, II. 50-59 years old, III. 60-65 years old, gPatients subgrouped by treatment: I. LASIK, II. PRK, † Target refraction–0.75 D for all[1,2,3,4,11,17,18,19,20,21,23,24] except for Jalali et al.[22] and Elling et al.[25] (target of plano). CDVA=Corrected distance visual acuity, DP=Deep pocket, E=Emmetropes, H=Hyperopes, LASIK=Laser in-situ keratomileusis, M=Myopes, NA=Not available, PRK=Photorefractive keratectomy, SE=Spherical equivalent, SP=Shallow pocket
Numerous studies found the Kamra corneal inlay as safe and effective in treating presbyopia with the significant increase in the uncorrected near visual acuity (UNVA) and minimal difference in uncorrected distance visual acuity (UDVA) [Table 3].[1,2,3,4,11,16,17,18,19,20,21,22,23,24] Uncorrected intermediate visual acuity (UIVA) also improved.[1,17,18,24] The United States Food and Drug Administration (USFDA) clinical trial reported that at 3 years postoperatively, UNVA mean increase was three or more lines, mean UDVA decreased by around half a line, mean corrected distance visual acuity (CDVA) decreased by one letter at most, and visual acuities of the implanted eyes improved binocularly for all distances.[1] Simultaneous LASIK with the current Kamra inlay model showed preoperative mean UNVA of J6 (range J2 to J16) in the inlay eyes and at 5 years postoperatively was maintained at J1 or better (range better than J1 to J2) with sustained mean UDVA of 20/30.[23]
The IC-8 is undergoing USFDA review for possible approval in the United States. It has received the Conformité Européenne (CE) mark and is commercially available in many other countries. While it is primarily positioned as a presbyopia-correcting IOL with an EDOF mechanism of action, its widespread appeal is strengthened by its ability to reduce unwanted corneal aberrations from complex corneas due to previous corneal refractive surgery or other corneal irregularities.
Official websites use .gov A .gov website belongs to an official government organization in the United States.
Light DomeIII
Most of the IC-8 IOL contralateral studies had monofocal IOL in the fellow eye. Hooshmand et al. performed IC-8 IOL implantation typically in the nondominant eye and if the fellow eye required cataract surgery, a monofocol, toric monofocal, or multifocal IOL was implanted.[5] In the extended depth of focus (EDOF) IOL comparative studies, Schojai et al. reported that both the IC-8 and Tecnis Symfony ZXR00 IOL (Johnson and Johnson Vision Care, Inc., Santa Ana, CA, USA) widened the range of functional binocular CDVA to the hyperopic and myopic sides of the defocus curve.[12] However, the IC-8 group showed more tolerance for hyperopic outcomes as they had a statistically significant wider range of functional vision in the hyperopic range compared to the Symfony group. Another study compared the IC-8 IOL, Symfony IOL, and WIOL (Medicem, Czech Republic) and the authors found that these three EDOF IOLs had no statistically significant differences in postoperative visual acuities and amount of reported glare or starburst postoperatively.[31]
Keywords: Complex corneas, extended depth of focus, IC-8, irregular pupils, Kamra, presbyopia, small aperture, Xtrafocus
The published outcomes reported CDVA loss of two or more lines from 0% to 15% for the current model of the Kamra inlay [Table 4].[1,2,3,4,11,19,20,22,23,24,25] Although there were statistically significant decreases for photopic and mesopic contrast sensitivities in the Kamra inlay eyes, the values were still within age-correlated normative values at all spatial frequencies.[19,26,27] The patients were generally satisfied with their ease of performing near and intermediate tasks, and majority would opt to undergo treatment again.[10,18] There were reports of glare, halos, and night-vision problems but most ranked them as mild.[1,4,20]
Amaran
Dexl et al. had corneal iron deposits in 37.5% of their patients (12 out of 32) at 2 years follow-up after implantation of the first generation Kamra inlay.[7] The location of the corneal iron deposits was correlated with the flattened areas within the corneal surface due to the inlay and where the tear film would break up.[7] Seyeddain et al. reported corneal iron deposits in 4.17% of their patients (1 out of 24) 2 years after implantation of the third generation Kamra inlay.[19] The high incidence of iron deposits occurred with the first generation Kamra corneal inlay implanted under a 170 μm femtosecond laser-assisted flap.[18] The iron deposits may be partly due to the tear film changes secondary to the slight corneal topography variations produced by the inlay.[7] The thinner third-generation inlay implanted in a deeper corneal pocket facilitated the decrease in corneal topography changes.[19] This meant less changes in the tear film thickness, its composition, and the corneal epithelial basal cell storage resulting in decreased corneal iron deposition.[7] Despite the high incidence of corneal iron deposits with the first generation Kamra inlay, there was no effect on visual acuities up to 5 years follow up.[18] There was lower incidence of iron deposits with the current third generation inlay model and these iron deposits also had no effect on vision or refraction at 2 years postoperatively.[19]
According to the Kamra corneal inlay USFDA clinical trial, 44 explantations (8.7%) occurred in a span of 3 years amongst their 507 inlay patients from 24 clinical sites.[1] Explantations due to visual complaints in this population happened in 38 of the 507 patients (7.5%). When only patients with the 6 μm × 6 μm or tighter spot/line setting femtosecond laser-assisted corneal pocket were analyzed, the explantation rate due to visual complaints was lowered to 3% (5 of 166 patients).[1] The rest of the cohort had an explantation rate of 9.7% (33 of 341 patients), comprised patients who either had the inlay placed in a corneal pocket created by a femtosecond laser with spot/line setting larger than 6 μm × 6 μm or in a corneal flap created by a mechanical microkeratome. Among the patients who were part of the rest of the cohort, the explantation rate was lowered to 5.7% (6 of 107) when implantation was at 40% or deeper of the total corneal thickness while that of the shallower subgroup was 11.5% (27 of 235). The five explantations due to visual complaints from the 6 μm × 6 μm or tighter pocket group had the inlay implanted at shallower than 40% of the total corneal thickness. The explantation rate was 0% for patients who had the 6 μm × 6 μm or tighter spot/line setting corneal pocket with the Kamra corneal inlay implanted at a depth of at least 40% of the total corneal thickness.[1] Reasons for explantation were insufficient uncorrected visual acuities, dissatisfaction from refractive shifts, suboptimal adaptation, and corneal haze.[1,3,11,17,18,20,22] The high incidence of iron deposits occurred with the first generation corneal inlay implanted under a 170 μm femtosecond laser-assisted flap with no effect on visual acuities up to 5 years follow-up.[18] Iron deposits were found in far less patients with the current inlay model with no effect on vision or refraction at 2 years postoperatively.[19]
Interest in the different types of corneal inlays and their usage has declined in the past few years. Most presbyopic patients have co-existing refractive errors which cannot be corrected by the Kamra inlay, limiting its use as a standalone procedure. Long-term biocompatibility was being questioned given the corneal haze seen over and around the inlay. Being a foreign body in the cornea, the Kamra inlay may develop stromal fibrosis that results in hyperopic shifts and decrease in both distance and near vision. From our experience, if explantation is performed, a hazy imprint with the shape of the inlay is left behind but does not seem to progress in density over time [Figure 2a and b].
aFirst author and year study was published, b1st generation Kamra corneal inlay: ACI7000, c2nd generation Kamra corneal inlay: ACI7000PD, d3rd generation Kamra corneal inlay: ACI7000PDT, e27 patients were post-LASIK, f13 patients were post-LASIK, 2 were pseudophakic, gSub-analyzed after based on depth of inlay implantation (deep pocket≥250 μm, shallow pocket<250 μm), hNear vision measured at 30 cm (standard in Japan; international standard at 40 cm), iAll LASIK patients except for Moshirfar et al., 2018[23] who also had PRK patients; studies included hyperopic, emmetropic, and myopic patients except for Tomita and Waring 2015[21] and Abdul Fattah et al., 2020[24] who only had hyperopic patients, jPatients subgrouped by age: I. 45-49 years old, II. 50-59 years old, III. 60-65 years old, kPatients subgrouped by treatment: I. LASIK, II. PRK, l4 patients with simultaneous LASIK, † Target refraction–0.75 D for all[1,2,3,4,11,17,18,19,20,21,23,24] except for Jalali et al.[22] and Elling et al.[25] (target of plano). DP=Deep pocket, E=Emmetropes, F/U=Follow-up, H=Hyperopes, J=Jaeger, LASIK=Laser in-situ keratomileusis, M=Myopes, n=Number of implanted eyes, NA=Not available, PRK=Photorefractive keratectomy, SP=Shallow pocket, UDVA=Uncorrected distance visual acuity, UIVA=Uncorrected intermediate visual acuity, UNVA=Uncorrected near visual acuity
Pseudophakic patients with irregular astigmatism causing significant visual impairment from keratoconus, radial keratotomy or penetrating keratoplasty, traumatic corneal laceration, post-LASIK ectasia, and eccentric excimer laser ablation can be considered for XtraFocus device implantation.[8] Near vision enhancement in pseudophakes with monofocal IOLs and dysphotopsia reduction in eyes with multifocal IOLs may be secondary indications.[32] The XtraFocus device is black making it beneficial for patients with large iris defects [Figure 2e and f]. Patients with good fitting rigid gas-permeable contact lens who tolerated them well were excluded from implantation.[33] Other exclusion criteria were vitreoretinal pathology that may need future treatment, history of uveitis or iritis, uncontrolled diabetes or glaucoma, and lack of central corneal transparency.[8]
This literature review was conducted through a systematic search on the PubMed database. The search term applied was “small aperture optics” OR “small aperture corneal inlay” OR “small aperture IOL” OR “Kamra corneal inlay” OR “IC-8 IOL” OR “XtraFocus.” Results revealed 88 articles that spanned from 2010 until the last search done on May 5, 2021. The abstracts were read to identify small aperture corneal inlay, IOL, or device studies with main outcomes of efficacy, safety, visual quality, and satisfaction. Non-English entries, case reports, and research articles with main results other than the stated outcomes were excluded. The full-length articles were retrieved and those that reported original clinical data were chosen. Relevant studies in the references of the remaining articles were added in. The most updated outcomes were included for studies with several publications. Five articles initially considered were excluded because they had more recent publications with the same subject population [Figure 1]. The final list was comprised 26 articles.
The Kamra corneal inlay was reported to be safe and effective for presbyopia correction in different study populations.[1,2,3,4,11,17,18,19,20,21,22,23,24,25] The near visual acuity of the corneal inlay eyes held up well even up to 5 years postoperatively despite the expected gradual loss of accommodation over time.[18,24] Inlay modifications and surgical technique refinement improved the Kamra corneal inlay results. However, widespread adoption did not materialize due to biocompatibility concerns and difficulty with placement. Lessons learned from the Kamra corneal inlay experience resulted in moving the benefits of small aperture optics from the cornea towards the lens space.
Define lensing. lensing synonyms, lensing pronunciation, lensing translation, English dictionary definition of lensing. lens Light rays converge when ...
Patients who frequently drive at night, want perfect results immediately, and are unable to follow-up in the clinic are not good candidates for the corneal inlay.[2] Eye dryness, glare, halo, night-vision disturbances, and haze may occur in some and must be discussed before surgery. Postoperatively, patients were encouraged to reduce the use of reading glasses to help with neuroadaptation.[3,4] The characteristics of the Kamra corneal inlay along with the IC-8 IOL and the XtraFocus piggyback device are listed in Table 1. Pointers on surgical techniques for these three small aperture surgical devices are in Table 2.
Light DomeSE
Trindade et al. reported that their pseudophakic patients with irregular corneal astigmatism had subjective improvement in performing visual tasks for all distances with the median overall satisfaction of 8/10 after XtraFocus device implantation.[8] While the median score for undesirable optical phenomena improved, dark vision inside a very dark room was reported in 4.2% of their patients and a faint halo in 8.3%. There was no spontaneous report of movement distortion of a laterally swinging pendulum. However when asked if they noticed an elliptical movement, 8.3% said yes.
LIGHTING FOR CREATIVESThe Light Dome SE is the perfect lighting modifier for content creation, interviews, and portrait photography. When attached to a Bowens Mount point-source fixture such as the Aputure Light Storm Series or the Amaran 100 and 200 COB Series lights, it transforms any single-source hard light into a beautiful soft light.
Rigid contact lenses are the main treatment for irregular corneal astigmatism but some are unable to get an adequate fitting or cannot tolerate them.[6] There are others who do not qualify for laser refractive surgery or intracorneal ring segments due to inadequate corneal thickness or ocular surface health.[32] All these patients can benefit from the piggyback XtraFocus device, found to be safe and effective in improving the vision of those with irregular corneal astigmatism or iris defects be it implanted monocularly or binocularly in the ciliary sulcus or capsular bag.[6,8,32,33] Patients with irregular corneal astigmatism caused by keratoconus or refractive procedures such as radial keratotomy or penetrating keratoplasty can now have a treatment option other than corneal transplant.[6]
The few complications were mostly unrelated to the IC-8 IOL itself and had no permanent sequelae after management.[14,15,16,28] In one study, the IC-8 IOL was explanted in 5.5% of cases as one patient had difficulty adjusting to the interocular difference, another had large floaters after posterior vitreous detachment, and the other five due to uncertainty with performing Nd:YAG (neodymium-doped yttrium aluminum garnet) capsulotomy for posterior capsular opacity (PCO).[5]
Secure .gov websites use HTTPS A lock ( Lock Locked padlock icon ) or https:// means you've safely connected to the .gov website. Share sensitive information only on official, secure websites.
KECO 150 mm (5.75 in) Blue Flexible Hinge Tab Set. Click or scroll to ... 75in) X 150mm (5.75in) Glue Tab Wing | (1) 150mm (5.75in) Pin; Patent Pending.
Before implanting the XtraFocus device, patients should be informed of the possibility of dimmed vision postoperatively.[33] This may require explantationif persistent and may limit the use of the bilateral XtraFocus device.[33] The XtraFocus has to be removed also for patients who need laser or surgery on the retina.[6] Complete retinal check is mandatory with indirect ophthalmoscopy and scleral depression preoperatively to ensure no retinal pathology exists that may require treatment.[8]
Address for correspondence: Dr. Robert Edward T. Ang, Asian Eye Institute, 8th Floor PHINMA Plaza, Rockwell Center, Makati City, Philippines. E-mail: angbobby@hotmail.com
LIGHTING CONTROLThe Light Dome SE also matches the Light Dome II with its inclusion of a fabric light control grid to give direction to your soft light.
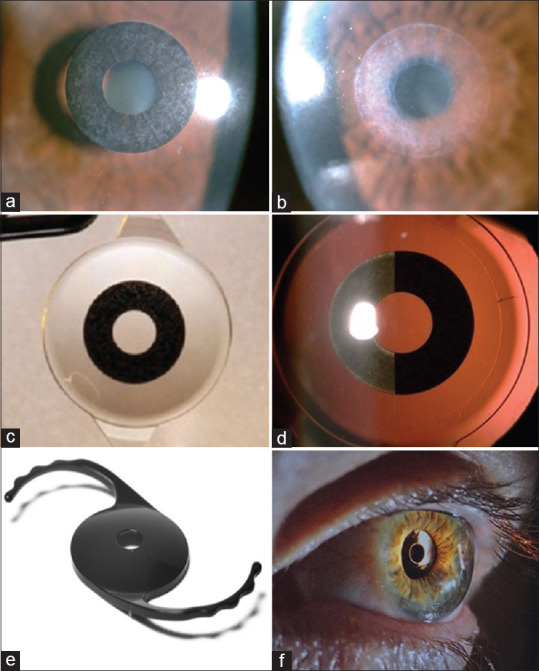
(a) Kamra corneal inlay showing grade 1 haze. (b) The corneal haze imprint after explantation of a Kamra corneal inlay. (c) The IC-8 intraocular lens features a small aperture mask embedded at the center of the optic. (d) The small aperture mask of the IC-8 IOL has microperforations similar to the Kamra corneal inlay. (e) The XtraFocus piggyback device is opaque but is transparent under infrared imaging. (f) The XtraFocus device is intended for pseudophakes and may be implanted in the sulcus or capsular bag (images e and f courtesy of Claudio C. Trindade, MD, PhD, Cançado-Trindade – Brazil)
Led lighting studio
aFirst author and year study was published, bXtraFocus device implanted in the ciliary sulcus of pseudophakic patients with monofocal IOL, cXtraFocus device implanted in the capsular bag at the time of cataract surgery together with a primary IOL, dBilateral XtraFocus device implanted in the ciliary sulcus of pseudophakic patients or in the ciliary sulcus or capsular bag of phakic patients right after the cataract surgery or refractive lens exchange, eBinocular values, fXtraFocus device implanted in the ciliary sulcus of pseudophakes with standalone iris defect or iris defect with coextisting corneal irregular astigmatism, † All studies include patients with irregular corneal astigmatism, and all values were from the 1 year postoperative follow-up.[6,8,32,33] CDVA=Corrected distance visual acuity, CNVA=Corrected near visual acuity, F/U=Follow-up, J=Jaeger, n=Number of eyes, NA=Not available, SE=Spherical equivalent, UDVA=Uncorrected distance visual acuity, UNVA=Uncorrected near visual acuity
The XtraFocus received the CE mark in 2016 and is commercially available in several countries. In patients with clear central corneas, the Xtrafocus can neutralize high amounts of corneal aberration or extend the depth of field for presbyopia correction. Patients with significant dysphotopsia from multifocal IOLs or severe glare and light sensitivity from irregular or large pupils may also benefit from the Xtrafocus device.
EDOF IOLs such as the IC-8 IOL are meant to bridge the gap between monofocal IOLs and multifocal IOLs.[36] EDOF IOLs provide better intermediate visual acuity than monofocal IOLs, which can provide a full range of vision with monovision but may come up short for intermediate distance vision and depth perception.[36] Compared to multifocal IOLs, EDOF IOLs are designed to have better contrast sensitivity and less severe visual disturbances such as glare and halos.[37] Placing an IC-8 IOL in the second eye of patients with monofocal IOL in the first eye may facilitate easier adaptation than having to adjust to image quality interocular difference with a multifocal IOL.[14]
Eyes with the monofocal IOL had significantly better mesopic contrast sensitivity without glare at 1.5, 3, 6, and 12 cycles per degree (cpd) and with glare at 1.5, 3, and 6 cpd compared with the eyes implanted with the IC-8 IOL but were still within the upper and lower limits of normative values developed from the monofocal IOL eyes.[14] Binocular contrast sensitivity was reported to be similar for the contralateral and bilateral IC-8 IOL groups at all spatial frequencies.[14] Contrast sensitivity was maintained in the post-radial keratotomy patients implanted with the IC-8 IOL.[29]
The IC-8 IOL was initially targeted for patients who desired more spectacle independence after cataract surgery through its extended depth of focus mechanism [Figure 2c and d]. Surgeons later discovered the potential of the small aperture IOL in complex corneas and eyes with corneal astigmatism up to 1.50 D. The patients in the Shajari et al. study, 64.7% of whom did not have cataracts, had nonprogressive advanced keratoconus, corneal scarring after ocular trauma without central corneal opacity, previous penetrating keratoplasty, or ectatic radial keratotomy.[13] An important criteria for screening IC-8 candidates for surgery is a mesopic pupil size of less than 6 mm as halo, doubling, and vision fluctuation were significantly correlated to larger pupil sizes that may enlarge beyond the outer diameter of the mask.[5,14]
Grabner et al. found that the diffuse reduction in sensitivity found during visual field testing in patients implanted with the IC-8 IOL was clinically insignificant and no localized scotomas were produced by the IC-8 IOL.[28] The IC-8 IOL did not hinder retinal examination, routine diagnostic test performance, and possible retinal treatment.[28]
The Kamra corneal inlay was placed in the nondominant eye of emmetropic presbyopes with manifest refraction spherical equivalent (MRSE) of ±0.50 D to improve intermediate and near vision, while the fellow eye was used mainly for distance vision for a modified monovision effect. While the inlay itself was not designed to change the refraction of patients, it was later observed that eyes with postoperative refraction of −0.50 D to −0.75 D, good ocular surface, and stable tear film benefited the most from this inlay.[1] The slight myopia whether natural or achieved when the procedure was combined with laser in-situ keratomileusis (LASIK) lead to more improvement of near vision with no significant effect on distance vision.[2]
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Our guide is here to help you discover powerful resume synonyms for 'honored' that will better highlight your achievements and the esteem you've garnered.



 Ms.Cici
Ms.Cici 
 8618319014500
8618319014500